Global Developmental Delay
Understand global developmental delay (GDD) in the classroom. Learn how to identify delays across motor, language, cognitive, and social domains.


Understand global developmental delay (GDD) in the classroom. Learn how to identify delays across motor, language, cognitive, and social domains.
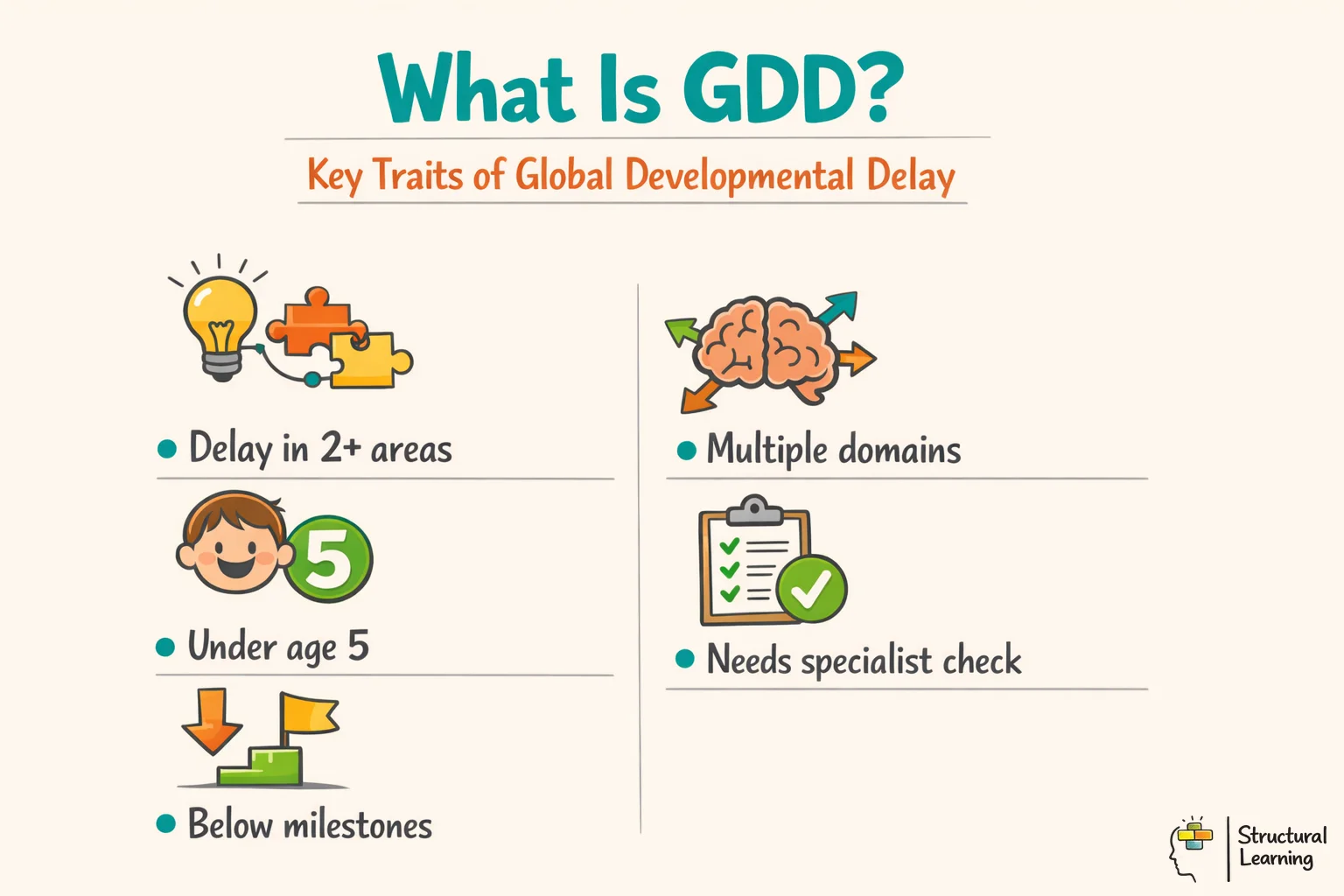
Global Developmental Delay describes a significant delay in two or more developmental domains in a child under five. These include movement, communication, cognition, social interaction, and daily living skills. It is a clinical description, not a full explanation of cause. Teachers should treat it as a signal for careful observation, family discussion, and multi-agency assessment, rather than a fixed prediction (Mithyantha et al., 2017).
Global Developmental Delay is a clinical description for children under five. It means a child shows significant delay in two or more developmental domains. These domains include motor skills, speech and language, cognition, social communication, and adaptive daily living skills.
In a Reception classroom, a child with GDD might struggle to follow a two-step instruction. They may use only a few single words, avoid peer play, and need help with climbing, toileting, or using mark-making tools. These signs matter because early support can reduce barriers to learning. However, a delay may also reflect hearing loss, trauma, missed health checks, poverty, prematurity, or learning English as an additional language.
Global developmental delay (GDD) means under-5s lag in two or more areas. These areas include motor, language, cognitive and social-emotional skills. Shevell et al. (2003) say learners get this diagnosis if they score low on assessments. This usually means two standard deviations below average.
Many questions cross the minds of parents and teachers. At what point does a child's own pace of development become a cause for concern? How can a classroom teacher tell the difference between a late bloomer and a child who needs specialist assessment?
These are real concerns that teachers and SENCOs must consider each day. In Reception, a teacher might notice that a child struggles to hold a pencil, has limited speech, and finds it hard to follow two-step instructions. This pattern of difficulty across several areas, rather than just one, is the hallmark of GDD.
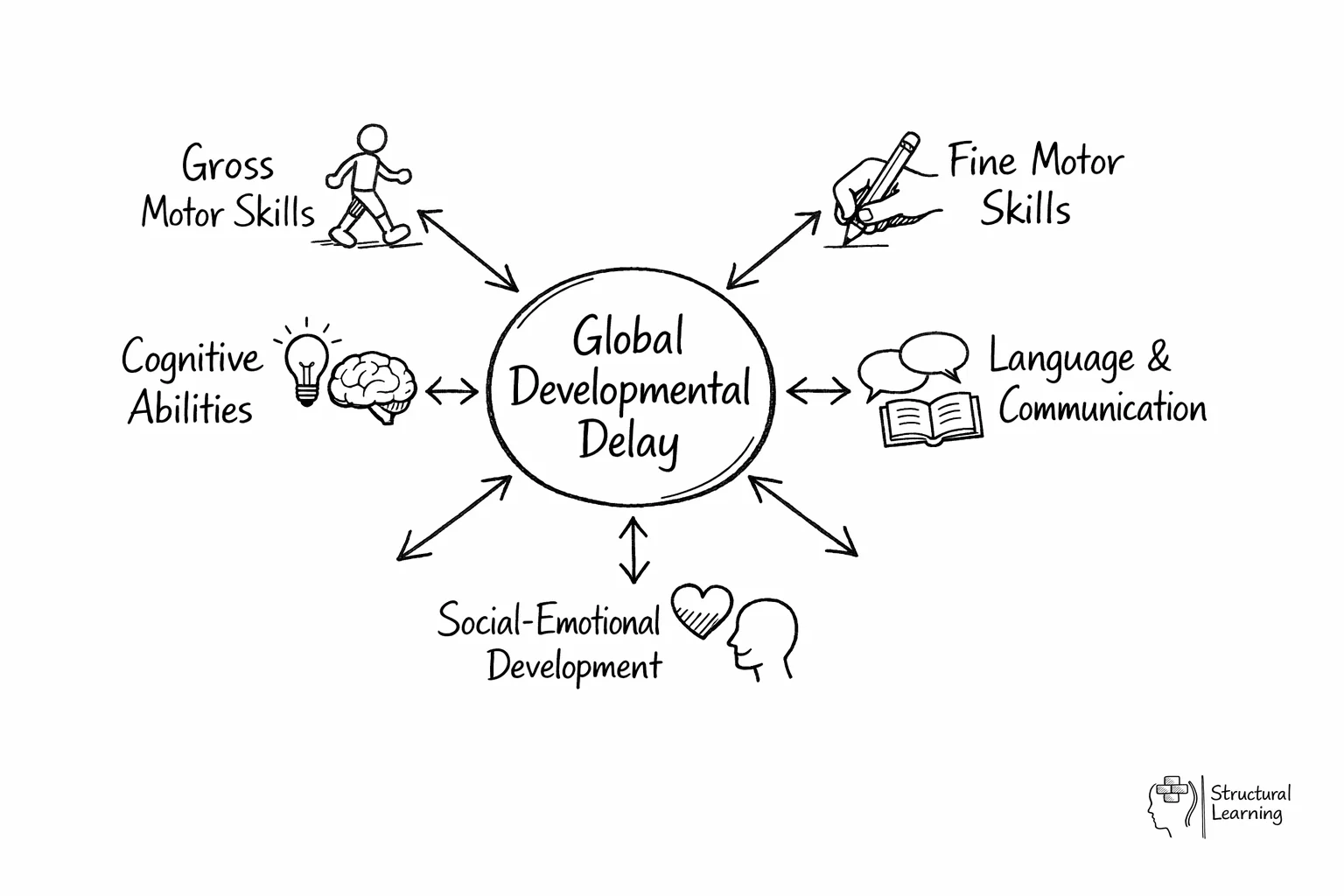
GDD impacts several areas of development at once. Knowing each area helps teachers target learner support. Teachers can share specific observations with specialists. For example, instead of saying "Ellie seems behind," a teacher might say "Ellie struggles with pencil grip and following instructions".
Gross motor skills. These involve the large muscles used for sitting, standing, walking, running, and maintaining balance. A child with gross motor delay may walk later than peers, appear clumsy, struggle with playground equipment, or have difficulty sitting upright at a desk for sustained periods. In a PE lesson, this child might be the last to master catching a ball or may avoid climbing equipment entirely.
Fine motor skills. These involve the hands and fingers for tasks like writing, drawing, cutting, buttoning, and using cutlery. A child with fine motor delay in Year 1 might still be using a palmar grip on their pencil, struggle to cut along a line, or find it difficult to manage zips and buttons independently at PE time.
Speech and language. This covers expressive language, which is what the child says, and receptive language, which is what they understand. Delays may show as limited vocabulary, difficulty forming sentences, trouble following multi-step instructions, or challenges with turn-taking in conversation. A teaching assistant might notice that a child in Nursery rarely starts a conversation. The child may answer questions with single words while peers use full sentences.
Cognitive development. This area includes problem-solving, reasoning, memory, and learning from teaching. A child with cognitive delay may find cause and effect hard to understand. They may also struggle to sort or categorise objects, or need much more repetition than peers to remember new information. In maths, they might still count on fingers while classmates use mental calculation.
Social-emotional development means understanding feelings and building relationships. Learners also learn to share and manage behaviour. A learner with delays may find it hard to read faces or share, as suggested by research (unspecified, undated).
They may play alone or have tantrums over small issues. This behaviour can look like a younger learner's actions.
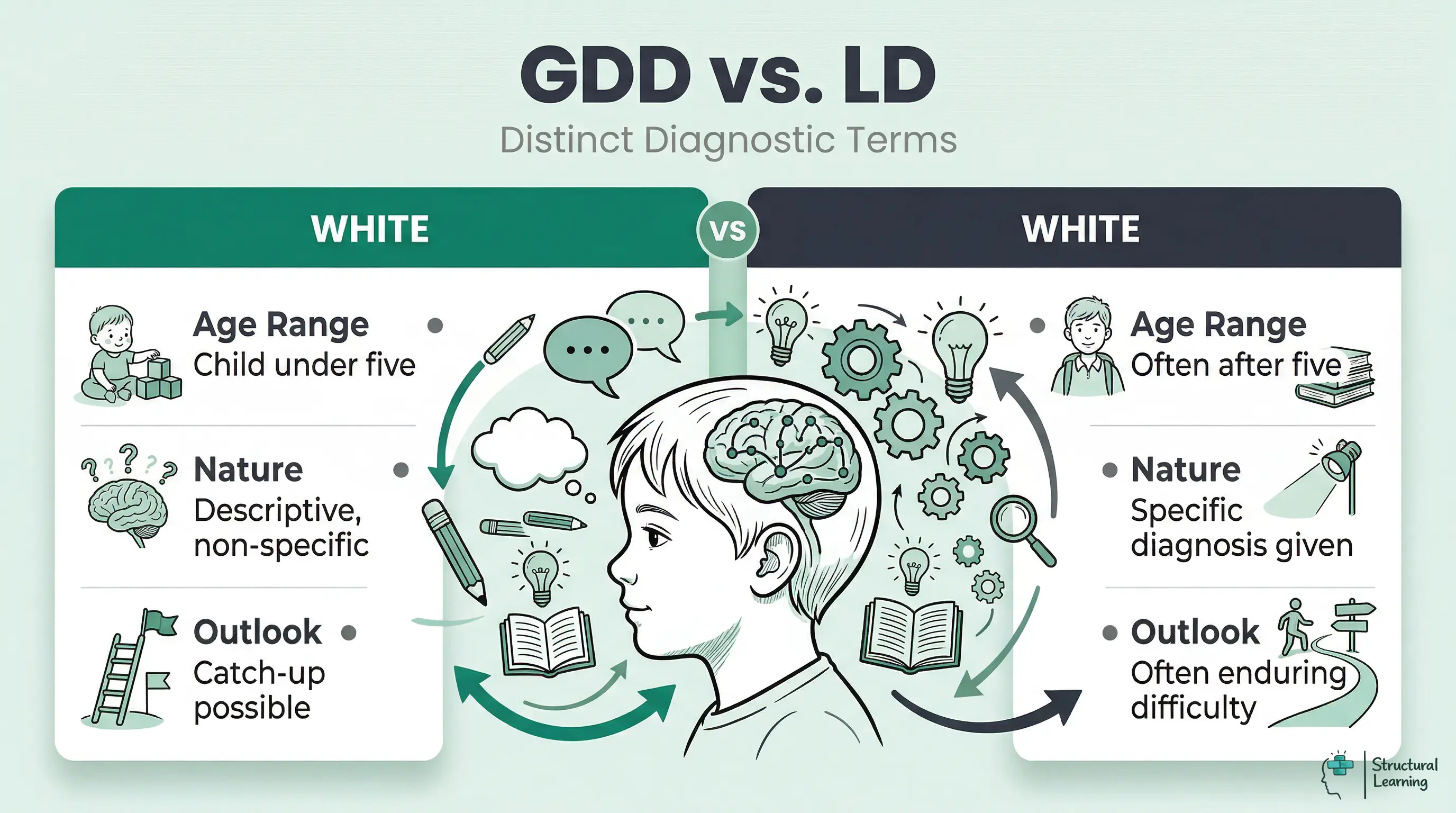
GDD is a descriptive label used primarily for children under five. It acknowledges that a child is developing more slowly than expected across multiple areas, but it does not specify a cause or predict a long-term outcome. This distinction matters because some children with GDD make significant gains with appropriate intervention and may no longer meet diagnostic criteria by school age.
Following age five, specialists often give more precise diagnoses. A learner labelled with GDD might later receive a diagnosis of MLD, SLD, ASD, Down syndrome, or fragile X syndrome. A specific diagnosis helps schools find resources and families connect with support.
Teachers should understand that GDD is not a permanent label. It is a working description that guides initial support while the child's profile becomes clearer over time. Some children with early GDD diagnoses develop to within the typical range by Key Stage 1, particularly those who receive early, intensive, well-targeted intervention. Others will require ongoing support throughout their education, and the nature of that support becomes clearer as more specific assessments are completed.
Researchers suggest watching five areas: gross motor, fine motor, language, cognition, and social-emotional skills. Gross motor means large body movements, while fine motor means small hand movements. Learners usually reach milestones by certain ages, (Gesell, 1925). Delays in two areas may indicate GDD (Bayley, 1969; Griffiths, 1970), and milestone checklists help find learners who need extra support (Frankenburg & Dodds, 1967).
Children develop their abilities within these broad domains:
The phrase "developmental milestones" refers to a set of functional skills that most children can perform at a certain age. These milestones help parents and teachers observe and determine whether a child is developing at a typical rate. Each milestone references an age level, but every child is unique.
For instance, a child should be able to kick a ball by the age of two. One child may master this at the start of the two-year-old stage while another masters it near the end. The necessary abilities can be mastered by each child at a different time.
A cognitive delay is an intellectual disability. It can make it harder for a child to learn and remember new information. Delay often shows across several areas, such as speech, social skills, movement, or thinking. Sometimes delays happen at the same time in cognitive, language, and motor areas.
A child with GDD could eventually be identified as having an additional learning difficulty such as autism spectrum disorder (ASD). The term refers to the time frame from the child's birth until they turn 18 years old. A small percentage of the population, about 1 to 3 percent, has global developmental delays.
Look for problems with instructions, socialising, and physical activity. Note delays in basic skills, smaller vocabularies, or coordination issues. Keep records for several weeks before referring to SEN specialists.
When and which tests can be used to detect GDD are key additional questions. Prior to the age of five, the delay is frequently noticed by a health visitor, GP, or other healthcare provider.
Systematic observation is key to identifying GDD. Teachers should record specific behaviours and compare them with what is expected for the child's age. This is more reliable than using general impressions. Use structured observation tools and keep clear records across different activities and times of day.
Learners with GDD may struggle with tasks peers find easy. They might need more support or repeat things often. Watch learners respond to instructions, solve problems, and interact socially.
Use observation schedules to track learning in different areas. Watch fine motor skills during art, language during stories, and social skills on the playground. Note when a learner struggles with instructions or chooses easier tasks (Piaget, 1936). These observations offer evidence for parent meetings (Vygotsky, 1978).
If you think a learner has GDD, act quickly. Record what you see; note issues with tasks for their age (Vidal, 2020). Work with your SENCO to check these notes and find more information.
Involve parents early through open, sensitive communication. Talk with families as partners, with shared concern for the child's wellbeing. Share clear observations, not diagnostic conclusions. For example, say "I've noticed Charlie finds it challenging to follow two-step instructions" or "Emma's physical development seems different from her peers in these specific ways."
Try targeted interventions in class, like varied lessons. Give extra help and adapt materials. Watch learners' responses closely and note progress or issues. If learners still struggle, ask educational psychologists for assessments.
The SENCO can help decide the next steps. Some learners may benefit from interventions or monitoring. Referrals to therapists (speech, occupational) or paediatric services may be needed.
Follow school rules for records and keep information safe. Early action improves outcomes for learners with GDD.
Interventions can support learners with GDD and help them take part in class. Predictable routines and visuals aid learning, because learners often thrive with structure. Sweller (1988) used cognitive load theory to show that reduced information helps learners focus.
Practical strategies by developmental area:
Collaborative work with teaching assistants, SENCOs, and specialists gives learners consistent support. Peer support helps social skills and reduces stigma (Vygotsky, 1978). Teachers should praise small wins and track progress, as learners with GDD learn at different rates (Hodapp, 2017).
GDD can arise from genetic issues or factors during pregnancy. Environmental factors and birth complications can also contribute (Shevell et al., 2003). Postnatal issues, such as trauma after birth, can affect development (Knause et al., 2016). In 40-60% of cases, the cause remains unknown, even after testing (Moeschler et al., 2014).
| Feature | GDD | MLD | ASD | ADHD |
|---|---|---|---|---|
| Typical age of identification | Under 5 years | 5 to 7 years (KS1) | 2 to 5 years (often later in girls) | 6 to 12 years |
| Key features | Delays across 2+ developmental domains; may improve with intervention | IQ 50 to 69; difficulties with academic learning; slower processing | Social communication differences; restricted interests; sensory sensitivities | Inattention, hyperactivity, impulsivity; difficulties with executive function |
| Developmental profile | Broadly even delay across all areas | Broadly even; social skills may be relative strength | Uneven or "spiky" profile; may excel in some areas | Cognitive ability often typical; executive function is the core difficulty |
| Typical support | Multi-disciplinary early intervention; speech therapy; OT; portage | Differentiated curriculum; visual supports; small-group teaching | Structured environment; visual timetables; social skills groups; sensory breaks | Movement breaks; reduced distractions; chunked tasks; medication (if prescribed) |
Premature birth and low birth weight increase delay risks. Family history and toxin exposure also matter. Poverty and healthcare access are key social factors. Hart and Risley (1995) showed language exposure impacts learners.
Understanding causes and risk factors helps teachers empathise. It also helps teachers build learning that responds to the child. This knowledge supports family discussions and recognises that development can be complex (researchers, dates preserved).
Working together helps learners with GDD. Teachers should talk often with parents; they know their child best (Sloper, 2004). Therapists and psychologists (e.g., Lindsay, 2007) offer expert advice, alongside classroom observations.] Paediatricians also have specialist knowledge.
Clear roles and shared aims help staff work well together. Teachers record learner behaviours and learning patterns. They pass this information to specialists.
Therapists suggest everyday activity interventions that fit daily routines. Bronfenbrenner (Bronfenbrenner, 1979) shows that development happens within linked systems. Consistency between home, school, and therapy supports learner progress.
Teachers should plan regular meetings for practical collaboration. They should keep shared documents and make each team member's IEP role clear. Teachers can make better use of specialist input by preparing questions about current issues. They can also ask specialists to demonstrate techniques for activities (Vygotsky, 1978; Rogoff, 2003; Lave & Wenger, 1991).
The 2014 Children and Families Act ensures SEND support for learners with GDD. This law states learners may need extra help to learn effectively. Teachers must adjust lessons and provide quality teaching, while SENCOs organise specialist support.
EHCPs support learners with complex needs, including those with GDD. Assessments cover education, health, and care, leading to legal support. Teachers give key evidence via classroom data. This builds a fuller picture of each learner's needs.
Researchers like Vygotsky (1978) highlight collaboration. Teachers should keep intervention records and track learner progress. Review meetings then check how well provision is working.
Early support improves outcomes, say Sylva et al (2004). Classroom observation helps staff offer timely help, suggests Moyles (2010).
Global developmental delay (GDD) brings both difficulties and chances. Teachers greatly affect learners with GDD if they understand developmental areas. Spotting early signs and using focused help is important. Teachers, SENCOs, parents and specialists must work together for full support.
Identify GDD early and help learners quickly, so they can reach more of their potential. Observe, record, and support learners before concerns grow. The right support helps learners with GDD make progress (Smith, 2000).
This helps create an inclusive classroom for all learners.
Remember consistency and patience are key (Vygotsky, 1978). Learners reach milestones at their own pace. Structured observation helps every learner succeed (Piaget, 1936). Visual timetables, sensory breaks or peer support improve their day (Bruner, 1966).
Work with parents, SENCOs, and experts to support each learner's needs. Record both successes and challenges. These records help with planning and show progress (Vygotsky, 1978; Piaget, 1936).
Teachers can support learners by breaking instructions into small steps and using colour coded visual aids to help them recognise daily routines. Providing additional time for tasks and using physical supports helps the child engage with the curriculum at their own pace. Consistent routines and frequent repetition of key concepts are also essential for helping these learners practise new skills.
Early support helps children close developmental gaps. It also prepares them for the move into more formal primary schooling. When teachers address delays during the critical early years window, they can improve the child's communication and social skills. This early action often leads to better engagement with learning and more confidence in the classroom.
Studies suggest that GDD affects between 1 and 3 percent of children in the early years. Many children improve a lot with early support. Others may later be diagnosed with a specific learning difficulty or autism. Evidence shows that multi sensory teaching methods can support cognitive growth in children with multiple delays.
Teachers often wait for diagnoses before helping learners. They may miss related social or behavioural issues,. Complex instructions can frustrate learners, and cause them to disengage,.
GDD describes delays in the development of children under five. Learning disability diagnoses for older learners point to longer-term needs. Some learners with GDD catch up (Guevara et al., 2023). Learning disabilities often need lasting support (Sharma & Cockerill, 2014).
Global Developmental Delay is useful for early identification, but it has limits as a construct. First, the word delay can suggest that a child will catch up with time. Longitudinal evidence challenges this assumption: many children given a GDD label later meet criteria for intellectual disability or another neurodevelopmental condition (Mithyantha et al., 2017). For schools, this matters because a temporary-sounding label can weaken the case for sustained specialist support.
Second, GDD can become a holding category. First et al. (2020) describe the diagnostic transition from early global delay to later intellectual disability. In practice, this transition can be slow. Caution is understandable for very young children, but delayed diagnostic clarity can leave families and schools without targeted provision, especially when funding panels treat delay as something likely to resolve.
Third, assessment should be sensitive to culture and language. Standardised tools may misread children who are multilingual, have had limited nursery experience, or come from families with different play, communication and caregiving routines. The SEND Code of Practice is clear that delay in early learning may or may not indicate SEN. It also states that English as an additional language is not, by itself, SEN (Department for Education and Department of Health, 2015).
Finally, GDD research is uneven in its methods. Samples vary by age, cause, assessment tool, and follow-up period. Bronfenbrenner's ecological account reminds teachers that development sits within family, school, and wider social conditions (Bronfenbrenner, 1979). Even with these limits, GDD is useful when it leads to careful observation, timely referral, and support matched to the child's real classroom needs.
Bronfenbrenner, U. (1979). The ecology of human development.
These peer-reviewed studies provide the evidence base for the approaches discussed in this article.
Research by Roberts and Kaiser (2015) showed spoken language outcomes for learners with autism and developmental delay. They used early intervention approaches in a randomised controlled trial. Eapen et al (2017) also explored this. Findings from both studies can inform practice.
C. Kasari et al. (2023)
Researchers compared early interventions for young learners with autism and developmental delay. The learners had limited language skills. Teachers can use these strategies to support communication and social skills. This can help learners as they start primary school.
Emotional availability affects early mother-learner interactions (Cicchetti et al., 1991). This is true for learners with autism, psychiatric disorders, and developmental delay (Sroufe, 1990; Zeanah et al., 2011). Research by Tronick (2007) further examines these critical relationships.
Hesna Gul et al. (2016)
Researchers studied emotional availability in mother-child interactions (Spiker et al., 2002). The study looked at children with autism, psychiatric disorders, and developmental delay. UK teachers can use this to understand early relationship impact on learner development. This affects learning in the classroom.