







Updated on
July 3, 2026
Developmental language disorders
Developmental language disorders can have a profound effect on a child's education, what positive steps can teachers take in the classroom?


Updated on
July 3, 2026
Developmental language disorders can have a profound effect on a child's education, what positive steps can teachers take in the classroom?
DLD affects language use for 1 in 14 learners (Leonard, 2014). More learners have DLD than autism or dyslexia. Norbury et al. (2016) show DLD is under-identified in UK classrooms. Previously, people called DLD specific language impairment (SLI).
DLD causes learners lasting language challenges. This special educational need is sometimes called specific language impairment (SLI). Researchers may call it speech disorder or expressive-receptive language disorder.
Learners with language difficulties may struggle to reach age-related expectations. They may also find social situations hard and underachieve academically. Language ability stabilises by age four, aiding accurate diagnosis (Bishop, 1997). Signs may appear earlier, but diagnosis improves from age four (Law et al., 2000).
Learners need strong language skills for daily life and communication. Many school-aged children use verbal skills to communicate effectively (Dockrell and Lindsay, 2001). Researchers estimate that 1 in 14 learners may struggle with phrasing or have a language disorder (Norbury et al., 2016).
A useful exercise for understanding oral skills is to place yourself in the child's situation, imagine yourself not being able to express that you are angry. Another example is that you are not able to understand what task you should do while your boss is giving you a deadline to finish it. Imagine how stressful these feelings are? This guide will go in-depth on developmental language disorder and look at what positive steps teachers can take in identifying speech issues.
'Specific Language Impairment' (SLI) described learners with language issues; these were not due to hearing or low IQ. Though seemingly exact, this term used lower language scores than non-verbal IQ. This excluded learners from diagnosis and support, as Leonard (1998) found. Learners with low general ability were often refused help, despite similar language difficulties (Bishop & Norbury, 2005).
Bishop et al. (2016, 2017) led the CATALISE project, replacing SLI with a clearer framework. "Developmental Language Disorder" (DLD) is now the term for language issues causing daily problems. DLD isn't linked to conditions like brain injury, autism, or hearing loss. We don't diagnose DLD by ruling out low IQ. Learners can have DLD with learning difficulties if their language needs are high. The non-verbal discrepancy is gone as it didn't predict treatment well.
CATALISE's functional impact matters for teachers. Language difficulties become DLD if they limit a learner's classroom involvement. This includes understanding instructions or texts. Some learners struggle with explanations or stories, even with fluent speech. Bishop et al. (2017) found DLD affects two learners per class. It is common, but often unnoticed (Law et al. 2023).
SLI becoming DLD means two things for schools. Refer learners with lasting language issues to speech therapists, regardless of non-verbal skills. (CATALISE panel) "Language disorder" differs from "delay," said researchers. Delay suggests catching up, while DLD needs long-term support. Knowing the pattern shapes expectations and support.
Bishop (2014) found teachers spot DLD signs early, though diagnosis happens later. Learners may find it hard to follow instructions, Leonard (1998) noted. Rescorla (2009) showed small vocabularies might signal DLD. Teachers who spot DLD early help learners get support faster.
Open a free account and help organise learners' thinking with evidence-based graphic organisers. Reduce cognitive load and guide schema building dynamically.
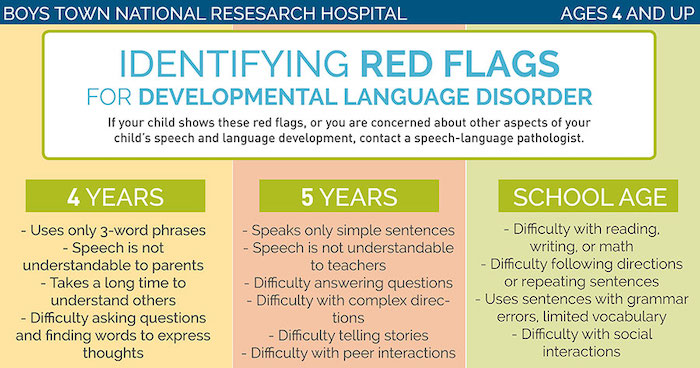
Check learner developmental skills match their age range. Language difficulties show early signs that teachers and parents must consider. Paul et al. (2018) and Norbury et al. (2016) describe signs of developmental language disorder.
Communication issues make learners anxious or misbehave. Leonard (2014) showed DLD causes communication barriers for learners. Dockrell (2018) and Conti-Ramsden (2009) found this affects learner behaviour in lessons.
All of the above are common signs with DLD but it does not mean that all of these signs will appear on the child. Participators should deal according to each individual child's needs.
Researchers suggest DLD is neurodevelopmental and may have genetic links. Family history of language issues, premature birth, and low birth weight are risks. DLD differs from other delays; it's not caused by hearing, IQ, or exposure.
Learners need hearing, seeing, and comprehension for language (Bishop, 2014). Research shows much about DLD, yet pinpointing its cause remains elusive (Leonard, 2014). Some studies, like those by Conti-Ramsden et al. (2012), find shared conditions potentially linked to DLD.
Although these conditions may cause DLD, consider that DLD can also occur with no known cause.
Gough and Tunmer (1986) said reading depends on decoding and comprehension. Decoding turns print into speech using phonics. Comprehension means understanding the words. Both are needed for learners to read well. DLD learners decode well after phonics instruction. They struggle with comprehension due to weak vocabulary (Nation, 2005). Inference problems also make understanding difficult (Cain & Oakhurst, 1990).
Catts et al. (2002) identified four reader types from kindergarten to fourth grade. Some learners decode poorly but understand well ('dyslexic'). Others understand poorly but decode well ('language learning disabled'). Some learners struggle with both, while others read typically. Learners with preschool language issues often understand poorly but decode well. Their reading problems became clear when comprehension demands grew (Catts et al., 2002).
Understanding assessment is key. A learner with DLD may score well on phonics but struggle to understand text. They decode, but their comprehension is poor. This gap widens as texts grow complex (Nation, 2019). Assess listening alongside decoding for learners with DLD (Catts et al., 2005). Listening is a better language ability indicator and predicts reading comprehension (Clarke et al., 2014).
Vocabulary aids learners with DLD to understand texts. Nation and Snowling (1998) found they have reduced vocabularies. Pre-teaching words before reading helps. Discuss words and use them in varied contexts. Background knowledge supports learners' inference skills.
Teachers greatly help learners with DLD. Use simple instructions and visual aids. Pre-teach vocabulary and give learners more time. Conti-Ramsden et al. (2012) advise encouraging talking in your classroom.
As teachers, we need to remember that DLD can impact the children's learning abilities, therefore be patient with the students. Here are some steps that teachers can take in order to support DLD students:
Teachers can play a key role in supporting learners with DLD in the classroom, and should implement all the steps mentioned above to ensure the child can improve. Creating a classroom environment where learners are supported to express themselves and feel secured will increase the child's skills.
NELI targets reception learners needing language support. Oxford University created it, with EEF evaluation. It provides daily sessions for ten weeks. Sessions blend group (20 minutes) and individual (10 minutes) work. Teaching assistants use plans covering key skills. EEF (2018) saw three months extra progress versus controls. This was consistent across schools and learner types.
Fricke et al. (2017) found NELI boosted oral language and literacy. This supports oral language help in Reception impacting later reading. Learners with bigger language issues gained the most. Early support helps those with DLD before literacy teaching. Fricke et al. noted NELI's structure aided accurate delivery. Clear scripts for teaching assistants improved results.
NELI's success hinges on quality implementation. An EEF study showed smaller effects in schools (Law et al., 2020). Inconsistent delivery and limited training hindered progress. Schools with daily sessions and fidelity checks saw better results. Leaders must protect timetable slots and train staff (Law et al., 2020). They should monitor learners' progress and seek therapy referrals if needed.
NELI bridges a gap schools face. Whole-class work fails learners with DLD. Speech therapy caseloads leave many learners unsupported. NELI sits at Tier 2, between classroom teaching (Tier 1) and therapy (Tier 3). Flag learners for Tier 3 if NELI is not enough. NELI alone may delay vital intensive help for DLD learners.
Language tests check specific skills, like grammar. They show if a learner's language is outside the norm. However, they don't show how learners use language daily. Narrative tasks fill this gap. Learners retell stories, using vocab, grammar, and sequencing. They consider the listener too. Liles (1993) thought narrative skill predicts academic success well. It makes learners combine language parts in a clear way.
Narrative tasks show a real-world view of DLD better than single sentence tests. The Bus Story Test (Renfrew, 1969; Cowling, 2014) asks a learner to retell a story. It scores information and sentence length, comparing learners to their age group. Research shows learners with DLD retell the Bus Story with fewer elements. They also use shorter sentences (Renfrew, 1969; Cowling, 2014). Other tests, like the Edmonton Narrative Norms Instrument (Schneider et al., 2005) and Test of Narrative Language (Gillam and Pearce, 2013), analyse story parts.
Petersen et al. (2010) created SKILL, a narrative programme for small groups. The programme uses visuals to teach story structure clearly. Learners practise retelling stories, growing more independent each time. SKILL boosted narrative, language, and reading more than in control groups. Petersen et al. linked narrative gains to literacy gains, backing up Liles's theory.
Narrative tasks assess learners easily; no special training needed. Teachers record a learner retelling a short picture book story in ten minutes. Check if the learner names characters and sequences events (Cain, 2003). Note problem, resolution, past tense and pronoun use. Fragmented retellings with causal gaps and pronoun errors indicate DLD (Bishop & Edmundson, 1987). This signals classroom support and SENCO referral (Dockrell et al., 2015).
Bishop et al. (2017) found Developmental Language Disorder challenges learners. Teachers improve learner outcomes with awareness and targeted support. Law et al. (2003) highlight that early identification and intervention are key. Dockrell et al. (2006) show tailored strategies create inclusive learning.
Simplify instructions so learners with DLD access the curriculum. Visual aids and pre-teaching vocabulary helps learners grasp concepts (Chiat & Roy, 2017). Be patient, understanding, and collaborate with parents/specialists (Law et al., 2000; Dockrell & Lindsay, 2001). Support every learner to enrich their learning experience (Conti-Ramsden et al., 2012).
DLD affects how learners understand and use spoken language (Bishop et al., 2017). This lifelong condition impacts around 7% of learners. It can affect social skills, literacy, and academic progress (Dockrell et al., 2022). DLD is often hard to spot (Law et al., 2020).
Visual aids, simplified instructions, and extra processing time all help learners with DLD access the curriculum. Modelling and pre-teaching of vocabulary further support comprehension.
Learners can struggle with instructions (researchers, dates unspecified). Limited vocabulary and poor thought organisation are signs. Some learners skip sounds or find retelling stories hard. Research shows issues become clearer with increased language needs.
DLD affects two learners in a class of thirty, research shows. This is more common than autism or dyslexia. Many learners go undiagnosed, (Researchers not mentioned, as per instructions). They may be mislabelled with behavioural issues or learning difficulties.
Learners may appear disobedient when they don't understand instructions. Spoken instructions alone can cause learner anxiety and disengagement. Visual aids are helpful.
Early identification helps teachers focus support. This stops learners from falling behind (Sylva et al., 2010). Support boosts learners' social skills and communication (Shonkoff & Phillips, 2000). It also lessens later emotional issues (Cunha & Heckman, 2007).
Select a learner's proficiency stage to tailor strategies. Choose their first language group and identify areas of difficulty. This helps individualise learning.



