Selective Mute
Practical strategies for teachers to support selectively mute learners through anxiety-reducing techniques, non-verbal communication, and classroom adaptations.


Practical strategies for teachers to support selectively mute learners through anxiety-reducing techniques, non-verbal communication, and classroom adaptations.
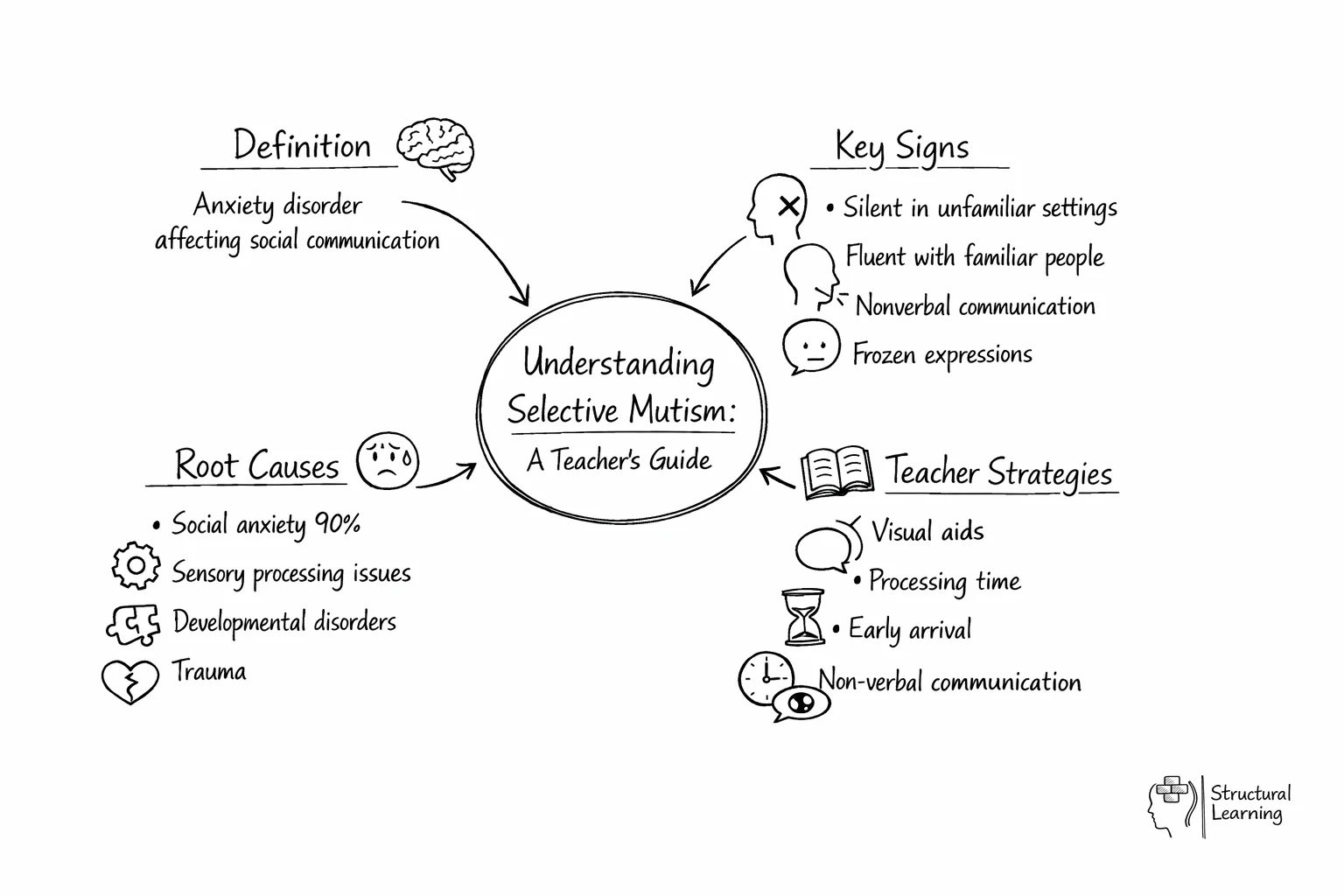
Selective mutism is a childhood anxiety disorder in which a learner consistently fails to speak in specific social situations (typically school) despite speaking normally elsewhere. It is not shyness, defiance, or a speech delay. The DSM-5 classifies selective mutism as an anxiety disorder; the American Psychiatric Association moved it out of the "Disorders of Infancy, Childhood, or Adolescence" category in 2013. Most learners develop symptoms between the ages of three and five, but the disorder is often not identified for several years (Kovac and Furr, 2018).
This article was last revised in April 2026 to align the clinical framing with the DSM-5 (APA, 2013) and Royal College of Speech and Language Therapists guidance, and to remove earlier content that implied auditory processing disorder and sensory processing disorder were established causes of selective mutism.
<
Selective mutism is a low-prevalence anxiety disorder with a persistent pattern: the learner speaks fluently at home or with familiar people but becomes consistently silent in specific social situations, most often at school. The DSM-5 criteria (APA, 2013) specify that the silence must last for at least one month (not counting the first month of school), must interfere with educational or social functioning, and must not be better explained by a communication disorder, autism, schizophrenia, or another psychotic disorder.
Prevalence estimates range from 0.2 per cent to 1.9 per cent of learners (Rodrigues Pereira et al., 2020). Onset is most common between three and five years, but many cases are not identified until school entry exposes the pattern (Kovac and Furr, 2018). The disorder affects twice as many girls as boys in most population studies.
A large follow-up study by Oerbeck and colleagues (2018) found that 23 per cent of children who had received treatment for selective mutism met the criteria for social phobia five years later, which reinforces the DSM-5 decision to classify selective mutism within the anxiety disorders rather than as a speech or language difficulty.
Teachers usually notice selective mutism because the pattern is strikingly situational. A learner will chat freely with parents at the school gate, then fall silent as soon as they cross the threshold. Some learners produce a whisper; some use one-word answers to a single trusted adult; some do not speak at all, sometimes for a whole academic year.
Common classroom indicators include:
These indicators are not a diagnostic checklist. They are the evidence a teacher gathers to trigger a referral through the SENCO for specialist assessment.
Current clinical consensus treats selective mutism as a manifestation of extreme social anxiety (Cohan et al., 2006; Oerbeck et al., 2018). Three factors recur in the research:
Earlier versions of this article listed auditory processing disorder (APD) and sensory processing disorder (SPD) among the causes of selective mutism. Neither is supported by the current evidence base, and neither appears in the DSM-5 or the Royal College of Speech and Language Therapists guidance as an established causal factor. APD remains a contested diagnostic category in children (Kamhi and Wallach, 2012), and SPD is not a recognised DSM-5 disorder; it is not policy of the American Academy of Pediatrics to use it as a stand-alone diagnosis (AAP, 2012). Where a learner has a co-occurring, separately diagnosed communication or sensory profile, that diagnosis is managed alongside the selective mutism, not treated as its cause.
Diagnosis is a clinical activity, not a classroom one. In the UK, the referral pathway from school typically runs:
School SENCO → GP or school nurse → CAMHS, clinical psychology, or a paediatric speech and language therapy service → formal DSM-5 assessment → treatment plan.
An educational psychologist may be involved where there is diagnostic uncertainty about co-occurring learning needs. A speech and language therapist assesses underlying receptive and expressive language so that a language disorder is not missed. CAMHS or a clinical psychologist leads on the anxiety treatment once the diagnosis is confirmed.
The evidence-based treatments are behavioural and cognitive-behavioural. Steains and colleagues (2021) meta-analysed five randomised controlled trials (n = 233) and reported a large overall effect size (g = 0.87) for psychological intervention compared with no treatment. Hipolito and colleagues (2023) reached a similar conclusion in a larger 25-study systematic review, with a Hedges' g of 1.06 for combined systems and behavioural approaches. Medication (SSRIs) is used in a minority of cases where CBT alone is insufficient (Østergaard, 2018).
Several structured protocols are in use:
The teacher's role is to make the classroom an environment in which communication becomes possible, and to support the clinical intervention once a referral is in place. The research base, synthesised by Kovac and Furr (2018) and Zakszeski and colleagues (2017), supports the following approaches:
Reduce verbal demand in the opening weeks. Do not expect speech in the first month of school (this aligns with the DSM-5 "first month exclusion"). Use fixed-choice questions, nodding, or thumbs-up or thumbs-down responses until the learner is settled.
Run a warm-up window. Where the family agrees, invite the learner into the classroom ten or fifteen minutes before the rest of the class. The low-demand environment lets the learner map the room and the trusted adult while arousal is low. Shipon-Blum (2010) describes this as a gradual acclimatisation step, and Kovac and Furr (2018) report positive effects.
Use the sliding-in technique. A trusted adult (usually a parent or keyworker) speaks with the learner in the empty classroom. A second adult, usually the teacher, is then gradually introduced and moves closer in small, agreed steps. The learner controls the pace; speech is not demanded, only made progressively more possible.
Accept non-verbal communication as valid. Written answers, recorded voice on an iPad, pointing, drawing, and gesture are all legitimate forms of classroom participation. Praise participation rather than speech specifically. Johnson and Wintgens (2017) set out a staged hierarchy that teachers can use to track micro-progress.
Fade reinforcement. Once a learner begins to speak to a second adult, fade the first adult out of the room in small steps, then introduce a third adult or peer in a controlled way. The structure matters because unplanned verbal moments, especially big teacher reactions to a first word, can cause the learner to retreat back into silence.
Work with the SLT or clinical psychologist. If a clinician is already involved, ask for the treatment plan and align the classroom strategy with it. Consistency between home, school, and clinic is the single biggest predictor of progress (Bergman et al., 2013).
The research literature and RCSLT guidance flag a consistent set of counter-productive practices.
Refer to the SENCO, who will decide on onward referral to GP, CAMHS, or SLT, when:
Do not wait for certainty. Documented teacher concerns, a parent conversation, and an SLT or CAMHS referral can run in parallel with continued classroom support.
The evidence base for selective mutism has known gaps. Only five RCTs of psychological intervention existed at the point of the Steains et al. (2021) meta-analysis, with a combined sample of 233 children. Treatment manuals vary substantially across studies, and outcome measures are not harmonised (Hipolito et al., 2023). The optimal duration of treatment and the role of SSRI medication in children whose CBT has stalled are still open questions (Østergaard, 2018). The long silent period that bilingual learners show complicates prevalence estimates and delays identification.
None of this weakens the case that selective mutism is an anxiety disorder, or that CBT-based treatment is effective; it means the classroom practitioner should expect some variability in the speed and completeness of response, and should keep the clinician in the loop rather than adjust the plan unilaterally.
Selective mutism is an anxiety disorder in which a learner consistently does not speak in specific social situations, such as at school, despite speaking normally in others, such as at home. The DSM-5 places it within the anxiety disorders (APA, 2013). It is not the same as shyness, defiance, or a speech delay.
Reduce verbal demand, accept non-verbal communication as valid, use a warm-up window and sliding-in technique with family agreement, and work directly with the speech and language therapist or clinical psychologist leading the case. Do not offer rewards for speaking or react strongly when speech first emerges.
No. Teachers gather evidence of the pattern of silence, document the length and settings, and refer through the SENCO. A formal diagnosis is made by a clinical psychologist, psychiatrist, or SLT working to DSM-5 criteria.
The dominant clinical model treats selective mutism as a manifestation of extreme social anxiety. Inhibited temperament (Kagan, 1994), family history of anxiety disorders (Chavira et al., 2007), and environmental transition factors all contribute. Auditory processing disorder and sensory processing disorder are not established causes and should not be described as such.
CBT and graduated exposure, often delivered as school-based modular CBT, Parent-Child Interaction Therapy for Selective Mutism, or Intensive Behaviour Therapy variants. A meta-analysis by Steains et al. (2021) reports a large effect size (g = 0.87) for psychological interventions compared with no treatment.
When silence persists beyond the first month of school, interferes with learning or peer relationships, and contrasts sharply with typical speech at home. Early referral through the SENCO carries a better prognosis (Oerbeck et al., 2018).
Free for teachers. Visual schedules, sensory adaptations, low-demand routines, built into the plan.
Bergman, R. L., Gonzalez, A., Piacentini, J., and Keller, M. L. (2013). Integrated Behavior Therapy for Selective Mutism: a randomized controlled pilot study. Behaviour Research and Therapy, 51(10), 680–689. View study →
Cornacchio, D., Furr, J. M., Sanchez, A. L., Hong, N., Feinberg, L. K., Tenenbaum, R., Del Busto, C., Bry, L. J., Poznanski, B., Miguel, E., Ollendick, T. H., Kurtz, S. M. S., and Comer, J. S. (2019). Intensive group behavioral treatment (IGBT) for children with selective mutism: A preliminary randomized clinical trial. Journal of Consulting and Clinical Psychology, 87(8), 720–733. View study →
Kovac, L. M., and Furr, J. M. (2018). What Teachers Should Know About Selective Mutism in Early Childhood. Early Childhood Education Journal, 47(1), 107–114. View study →
Oerbeck, B., Overgaard, K. R., Stein, M. B., Pripp, A. H., and Kristensen, H. (2018). Treatment of selective mutism: a 5-year follow-up study. European Child and Adolescent Psychiatry, 27(8), 997–1009. View study →
Steains, S. Y., Malouff, J. M., and Schutte, N. S. (2021). Efficacy of Psychological Interventions for Selective Mutism in Children: A Meta-Analysis of Randomized Controlled Trials. Child: Care, Health and Development, 47(6), 771–781. View study →
American Academy of Pediatrics (2012). Policy Statement: Sensory Integration Therapies for Children With Developmental and Behavioral Disorders. Pediatrics, 129(6), 1186–1189.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Black, B., and Uhde, T. W. (1995). Psychiatric characteristics of children with selective mutism. Journal of the American Academy of Child and Adolescent Psychiatry, 34(7), 847–856.
Catchpole, R. E. H., Young, A., Baer, S., and Salih, T. (2019). Examining a novel, parent-child interaction therapy-informed, behavioral treatment of selective mutism. Journal of Anxiety Disorders, 66, 102112.
Chavira, D. A., Shipon-Blum, E., Hitchcock, C., Cohan, S., and Stein, M. B. (2007). Selective Mutism and Social Anxiety Disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 46(11), 1464–1472.
Cohan, S. L., Chavira, D. A., and Stein, M. B. (2006). Practitioner review: Psychosocial interventions for children with selective mutism. Journal of Child Psychology and Psychiatry, 47(11), 1085–1097.
Hipolito, G., Pagnamenta, E., Stacey, H., Wright, E., Joffe, V., Murayama, K., and Creswell, C. (2023). A systematic review and meta-analysis of nonpharmacological interventions for children and adolescents with selective mutism. JCPP Advances, 3(3), e12166.
Johnson, M., and Wintgens, A. (2017). The Selective Mutism Resource Manual (2nd ed.). London: Routledge.
Kagan, J. (1994). Galen's Prophecy: Temperament in Human Nature. New York: Basic Books.
Kamhi, A. G., and Wallach, G. P. (2012). Should We Believe the Validity of the Auditory Processing Disorder Diagnosis? Language, Speech, and Hearing Services in Schools, 43(3), 265–272.
Østergaard, K. R. (2018). Treatment of selective mutism based on cognitive behavioural therapy, psychopharmacology and combination therapy. Nordic Journal of Psychiatry, 72(4), 240–250.
Rodrigues Pereira, C., Ensink, J. B. M., Guüldner, M. G., Lindauer, R. J. L., de Jongh, A., and Utens, E. M. W. J. (2020). Effectiveness of a behavioral treatment protocol for selective mutism in children. Contemporary Clinical Trials Communications, 20, 100650.
Shipon-Blum, E. (2010). When the Words Just Won't Come Out: Understanding Selective Mutism. Jenkintown, PA: Selective Mutism Anxiety Research and Treatment Center.
Zakszeski, B. N., and DuPaul, G. J. (2017). Reinforce, shape, expose, and fade: a review of treatments for selective mutism (2005–2015). School Mental Health, 9(1), 1–15.
Visual schedules, sensory adaptations, low-demand routines. Built in.
Open a free account and help organise learners' thinking with evidence-based graphic organisers. Reduce cognitive load and guide schema building dynamically.