Updated on
July 2, 2026
Talk Boost: What Schools Need to Know
A practical guide for teachers and SENCOs on the Talk Boost intervention, covering who it's for, how it works, the evidence, and implementation challenges.


Updated on
July 2, 2026
A practical guide for teachers and SENCOs on the Talk Boost intervention, covering who it's for, how it works, the evidence, and implementation challenges.
Talk Boost is a structured, time-limited language intervention for learners with delayed, but not disordered, language development. Delivered in small groups by trained teaching assistants or early years educators, it aims to accelerate progress in core spoken language skills. This guide explains what the programme involves and which learners are the best fit. It also shows how to manage the practical challenges of running it in a busy school.
Talk Boost is a series of targeted language interventions developed by the UK charity Speech and Language UK. It is designed to be delivered in primary schools and early years settings by trained staff members, typically teaching assistants (TAs). The core purpose of the programme is to improve the spoken language skills of children identified as having delayed language development.
The intervention works by providing a block of intensive, regular support in small groups. Using a set of structured activities and resources, it focuses on developing fundamental skills that underpin both academic learning and social communication.
There are several versions of the programme:
In all versions, children are selected using a screening tool. They join several weekly group sessions led by a trained adult. Whole-class activities help them generalise their new skills.
Correctly identifying learners is the most critical factor in the success of any intervention. Talk Boost is designed for a specific subset of learners who are falling behind their peers in language development.
Talk Boost is for learners who:
The most common misconception is that Talk Boost is a catch-all solution for any child with a communication difficulty. The evidence and programme guidelines are clear that it is not suitable for all learners.
The Talk Boost intervention follows a systematic process designed to build language skills sequentially.
Screening and Selection: The process begins with the Talk Boost Tracker, an online screening tool. Teachers assess learners against a set of criteria to identify those whose language skills are behind the expected level for their age. The tracker helps pinpoint the specific areas of language a child is struggling with and confirms their suitability for the intervention.
Small Group Sessions: Selected learners take part in group sessions, typically held three times a week for around 30-40 minutes. These are led by a trained teaching assistant or educator in a quiet space away from the main classroom. The sessions are built around a series of structured activities, often involving a character or story to engage the children. For example, in Early Talk Boost, the activities are based around characters like Tizzy the Tiger.
Skill Development: The activities are carefully sequenced to build on each other. They cover core language components, including:
Classroom Transfer: A important part of the programme is a weekly whole-class activity led by the class teacher. This is designed to help the learners in the intervention group practise and apply their new skills in the context of the main classroom. It also has the benefit of reinforcing good language skills for all learners.
Parental Engagement: The programme encourages schools to involve parents by sharing information about what their child is learning. Resources like activity books are provided to help parents practise the skills at home, creating a vital link between school and home life.
Implementing Talk Boost effectively requires careful planning and coordination.
Secure Senior Leadership Buy-In: First, ensure the Senior Leadership Team (SLT) understands what resources are needed. This includes training costs, a dedicated quiet space, and timetabling for a trained staff member.
Identify and Train Staff: Select a teaching assistant or educator to be trained. This person must attend the official Talk Boost training delivered by a licensed tutor. Remember, this training cannot be cascaded to other staff members.
Timetable the Intervention: This is often the biggest hurdle. The school must commit to releasing the trained staff member for the required sessions each week. This must last for the full nine to ten weeks of the programme. A consistent, quiet, and distraction-free space must be allocated for the sessions.
Screen Learners: The class teacher uses the online Talk Boost Tracker to screen their whole class. This should be done carefully to ensure the correct learners are identified. The SENCO should oversee this process to ensure consistency.
Group the learners based on tracker results. Select up to eight learners for Early Talk Boost. For KS1 or KS2, choose four learners to form the intervention group. Inform parents that their child has been selected for this supportive programme.
Run the Sessions: The trained TA delivers the sessions as prescribed in the manual, following the structured activities. Fidelity to the programme is key to achieving the intended outcomes.
Monitor Progress: The tracker is used again at the end of the intervention block to measure progress. The SENCO and class teacher should review this data to evaluate the impact and decide on next steps for each learner. Some may have caught up, while others may require further support or referral to a specialist.
When considering any intervention, it is vital to look critically at the evidence. While Talk Boost is widely used, the evidence for its effectiveness is emerging and has some important limitations.
A 2025 review commissioned by the Department for Education (McKean et al.) identified Talk Boost as a targeted intervention with good-quality evidence. The review cited trial data showing that Talk Boost KS1 produced significant gains in expressive narrative skills for Year 1 learners.
However, other evaluations have raised questions. The core academic trial on Early Talk Boost (Reeves et al., 2018) found that while children made progress, the statistical impact (measured by Hedges' g) was very low. This makes it difficult to be certain that the progress was caused by the intervention rather than by natural development.
Furthermore, a large-scale efficacy trial funded by the Education Endowment Foundation (EEF) was cancelled in early 2024 due to significant implementation challenges in real-world school settings. This highlights the difficulty schools face in delivering the programme with high fidelity due to issues like staff turnover and timetabling pressures.
Many research reviews agree that small-group oral language interventions can be highly effective (Donolato et al., 2023; Heidlage et al., 2019). Good implementation is key. A trained adult must deliver the programme as designed to the intended learners. If schools increase group sizes, use untrained staff, or teach learners with complex needs, the programme becomes much less effective.
The ultimate goal of any small-group intervention is for the skills to transfer back into the whole-class environment. A teacher can use principles from Talk Boost to strengthen universal provision for all learners, particularly in vocabulary and comprehension.
This example shows how a Year 5 teacher could adapt Talk Boost KS2 principles for a geography lesson on coastal landscapes.
1. Activating Listening and Comprehension Monitoring
2. Scaffolding Vocabulary
This approach is inspired by the explicit instruction in Talk Boost. It helps move targeted strategies from the group into daily classroom culture. This benefits all learners.
Before committing to Talk Boost, use this checklist to assess if it's the right fit for your school and learners.
| Not Recommended For | Reason Why | Alternative Approach |
|---|---|---|
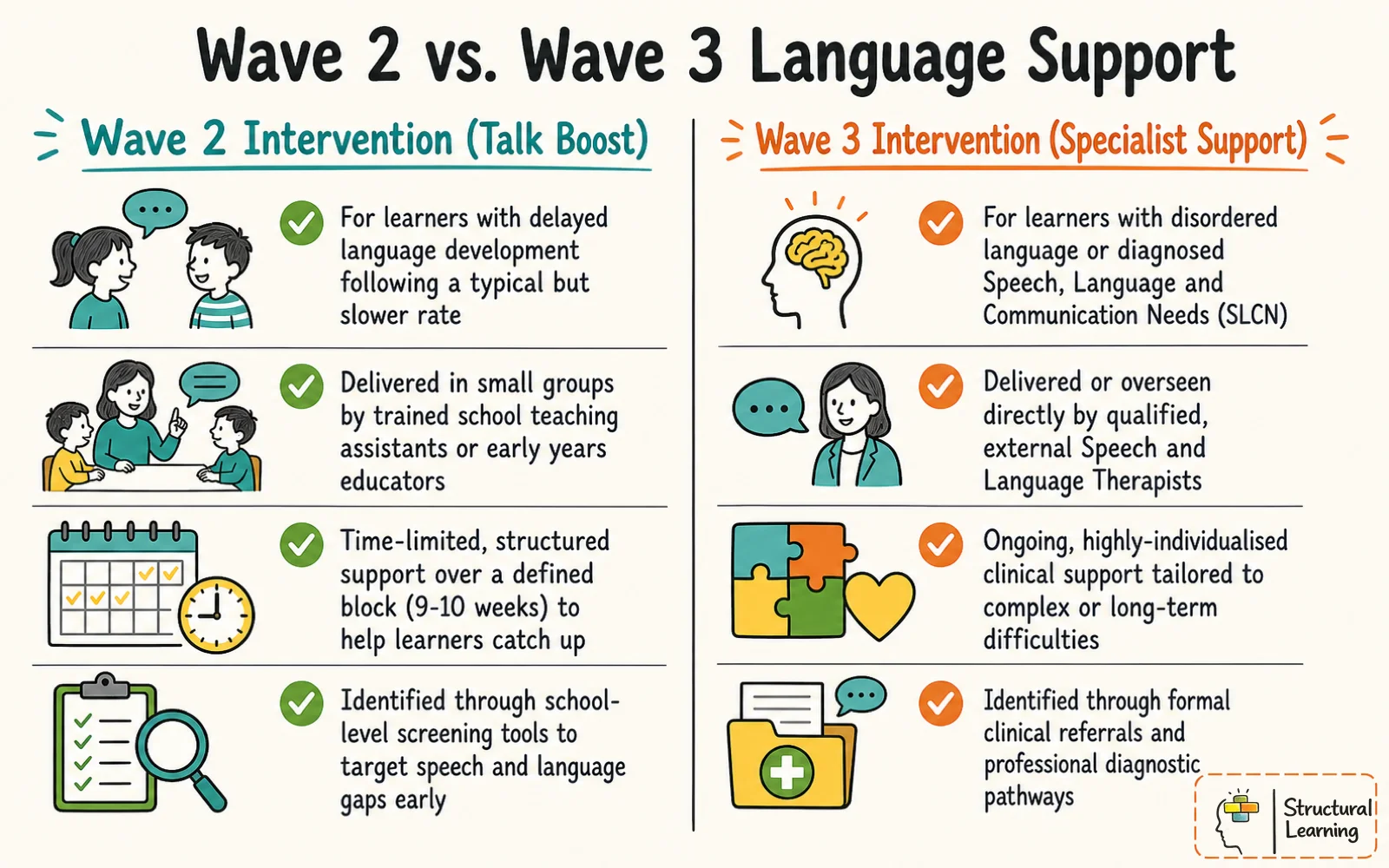
| Learners with diagnosed SEN | These learners require a more specialist, individualised, and long-term approach (Wave 3) than a 9-week group programme can provide. | Referral to a specialist Speech and Language Therapist (SLT) for diagnosis and a personalised therapy plan. |
| EAL learners (in early stages) | The programme is not designed for bilingual learners acquiring English. Their language profile must be assessed in their home language first to distinguish a language delay from a language disorder. | Focus on high-quality EAL provision, immersive language environments, and assessing skills in their home language before considering an intervention for a disorder. |
| Learners with suspected DLD | Developmental Language Disorder (DLD) is a significant, long-term condition. These learners need a formal diagnosis and specialist SLT support. | Use a DLD screening tool and refer to an SLT for a full assessment. |
| Whole classes or large groups | The intervention is designed and evidenced for small groups (typically 4-8 learners). The benefits are diluted in larger groups. | Use high-quality universal oracy and vocabulary strategies for the whole class, such as those embedded in Structural Learning's Talk Tactics. |
Learner Selection
Logistics and Resources
Implementation and Monitoring
Can't one trained TA just show the other TAs how to do it? No. Speech and Language UK explicitly forbids cascade training. The programme's effectiveness is linked to the quality of delivery, which depends on the official training.
Can we run it with a larger group to help more children? The programme is designed and evidenced for small groups. Increasing the group size will reduce the intensity and individual attention for each child, diluting the impact. It is better to run the intervention properly with one group than poorly with two.
What if a child is still struggling after the intervention? If a learner does not make expected progress after completing Talk Boost, it may indicate a more complex underlying need. This is the point at which to consider a referral to a specialist Speech and Language Therapist for a more detailed assessment.
How long does it take to see an impact? The programme is designed to show progress over its 9 or 10-week duration. The post-intervention tracker is the primary tool for measuring this change.
Start building comprehension monitoring into your whole-class teaching. Before explaining a new concept, explicitly tell your learners: "Your job is to listen carefully and to tell me if any part of my explanation is not clear. This simple instruction shifts the classroom culture from passive listening to active thinking. This core principle underpins the Talk Boost approach and benefits every learner.