The WellComm Speech and Language Toolkit is a widely used screening and intervention resource for identifying and supporting learners with language difficulties. It is designed for use with children from 6 months to 11 years of age, providing a structured approach to assessing language skills and offering targeted activities to address areas of need.
For many schools, WellComm is the first step in building a more systematic approach to speech and language support. It helps move practice beyond subjective teacher judgement to a more data-informed process. However, moving from the toolkit's traffic-light report to effective, manageable classroom action presents a significant challenge.
Key Takeaways
What it is: WellComm is a two-part toolkit featuring a screening assessment to identify potential language needs and an linked book of intervention activities.
Its Purpose: It is primarily a universal screener to flag learners who may require additional support. It is not a formal diagnostic tool.
The Challenge: The screening component has recognised limitations in its diagnostic accuracy and suitability for learners with English as an Additional Language (EAL).
The Solution: Effective use involves seeing the screening score as the start of an inquiry, not the final word. The intervention activities must be adapted and integrated into quality-first teaching rather than delivered in isolation.
What is the WellComm Toolkit?
The toolkit consists of two core components: a screening assessment and a bank of intervention activities.
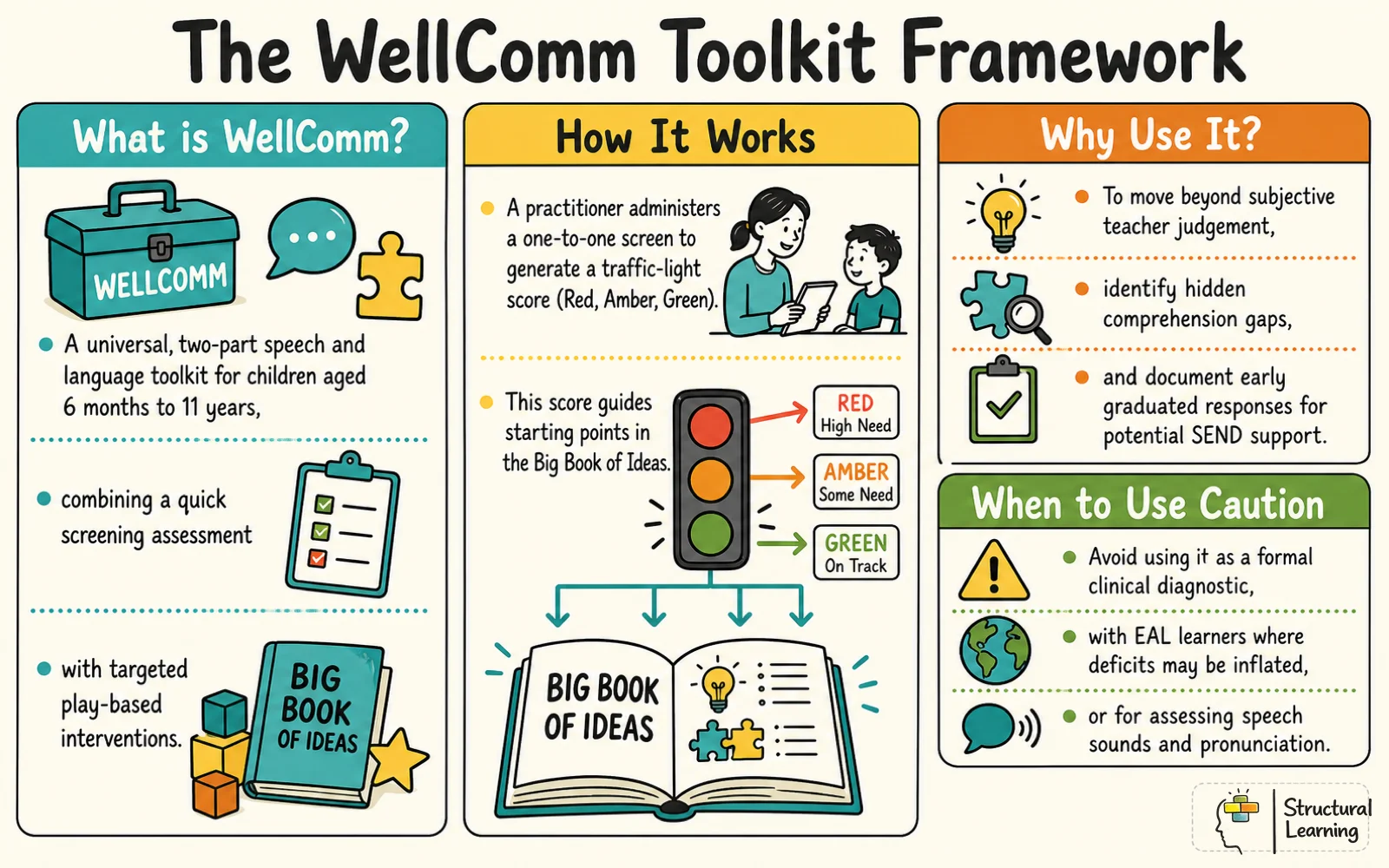
The Handbook (Screening): This contains the screening assessment itself. A practitioner (often a SENCO, teacher, or trained teaching assistant) administers the screen one-to-one with a learner. The assessment uses a series of questions and prompts to assess different aspects of language, primarily focusing on understanding and vocabulary.
The Big Book of Ideas (Intervention): This contains hundreds of play-based activities, categorised and linked to the assessment sections in the Handbook. Once a learner's needs are identified, the practitioner can turn to the corresponding section of this book for targeted intervention ideas.
The central process involves using the screening tool to generate a "traffic light" score, Red (significant delay), Amber (some delay), or Green (within expected range). This score then guides the practitioner to an appropriate starting point for intervention within The Big Book of Ideas.
Who is WellComm for? (And Who is it Not For?)
WellComm is designed as a universal screening tool. Its main strength lies in its ability to quickly survey a whole cohort and flag children who might have underlying language difficulties, including those who appear confident and articulate but may have hidden comprehension gaps (GL Assessment, 2021).
However, it is crucial to understand its limitations.
WellComm is a good fit for:
Settings that need a structured, off-the-shelf way to start screening for language needs.
Identifying learners who may have fallen below age-related expectations in vocabulary and language comprehension.
Providing a bank of ideas that can be adapted for small group work and classroom differentiation.
Informing and documenting the early stages of a graduated response for a learner with potential SEND.
Use WellComm with caution for:
Formal Diagnosis: It is not a diagnostic tool. A WellComm report alone is not sufficient for a speech and language therapy referral, though it can provide valuable supporting evidence of needs and interventions already tried (Pak et al., 2023).
Learners with EAL: The toolkit is normed on English speakers. Using it with learners who have English as an Additional Language can inflate their apparent deficits, as it assesses English language skills, not their cognitive potential or linguistic ability in their home language (Dysart and Code, 2024).
Assessing Speech Sounds: The screen does not evaluate a child's clarity of speech or pronunciation. It will not identify children with Speech Sound Disorders (SSD) unless their difficulty also impacts their vocabulary and comprehension (Dysart and Code, 2024).
How Does WellComm Work? The Five-Step Process
Implementing WellComm follows a clear, structured sequence. The goal is to connect the data from the screening to a specific, targeted action.
The Screening Assessment: The practitioner takes a learner to a quiet space and works through the relevant section of The Handbook. This takes around 15-20 minutes per child and involves asking questions and recording the learner's verbal or non-verbal responses.
Scoring and the Traffic Light System: The responses are scored to produce a raw score, which is then converted into the Red, Amber, Green traffic light rating. This gives a simple, visual indication of the learner's needs compared to age-related expectations.
Finding the Starting Point: The score report directs the practitioner to a specific section and activity number in The Big Book of Ideas. This ensures the intervention is targeted at the area of weakness identified in the screen.
Delivering Targeted Intervention: The practitioner uses the activities from The Big Book of Ideas to support the learner. These are designed as short, focused, play-based tasks that can be delivered in small groups or one-to-one.
Tracking and Monitoring Progress: After a period of intervention (typically a term), the learner should be re-assessed to measure progress and determine if further support is needed. This creates a clear cycle of assess, plan, do, review.
A Classroom Example: Integrating WellComm into a Year 5 Science Lesson
The real power of any intervention is its ability to enhance learning within the curriculum. The activities in The Big Book of Ideas should not be confined to withdrawal sessions. They provide a blueprint for the kind of language scaffolding that can be woven into everyday lessons.
The WellComm Toolkit Framework
This approach, embedding language support into high-quality continuous provision, is particularly effective for learners with identified language delays or those with SEND.
Here is a realistic example of a Year 5 teacher putting WellComm principles into action during a science experiment on filtration.
Language Target: Receptive and expressive use of temporal concepts ("before" and "after"). This is a common target in the WellComm framework and vital for understanding instructions and explaining processes.
Intended Learning Gain: To strengthen learners' ability to process and use chronological language, helping them to follow multi-step instructions and construct more precise scientific explanations.
What the Teacher Says: Pointing to the laid-out apparatus (a glass beaker, a plastic funnel, filter paper), the teacher deliberately avoids gesturing at specific items. "Look at our equipment. Which item must we place inside the funnel before we pour the liquid? And what will we do after we have set up the beaker?"
What the Learners Do: By removing non-verbal cues, the teacher ensures all learners must process the temporal language itself. Learners must listen, sequence the actions mentally, and then carry out the task. They can then be asked to explain the process back using the target vocabulary: "We must fold the filter paper before we put it in the funnel."
Evidence and Limitations: A SENCO's Guide to the Research
The evidence base for early language intervention is generally positive, suggesting that targeted support can improve outcomes (Feltner et al., 2024; Rodgers et al., 2024). However, the evidence for screening tools themselves, including WellComm, is more mixed and warrants careful consideration (Wallace et al., 2015).
SENCOs and school leaders should be aware of three specific critiques when interpreting WellComm data.
1. Low Diagnostic Accuracy
A 2025 rapid evidence review commissioned by the Department for Education (DfE) rated WellComm's diagnostic accuracy as "low" (McKean et al., 2025). The review highlighted studies showing the tool's specificity could be as low as 58.5%.
In a classroom context, low specificity means a high number of "false positives." Many learners who are flagged as Amber or Red may not have a genuine underlying language disorder. They may simply have had less exposure to the specific vocabulary or concepts assessed. This means the tool can lead to the over-identification of needs, creating unnecessary work and anxiety.
2. Limited Scope and Standardisation
Academic evaluations note that WellComm does not assess all aspects of language. Crucially, it does not evaluate speech sound production, meaning it can miss learners with Speech Sound Disorders (Dysart and Code, 2024).
Furthermore, the tool's developmental norms were not created from an independent standardisation sample but derived from previous literature. This, combined with its prescriptive English-normed design, makes it less reliable for assessing learners from diverse backgrounds, especially those with EAL or other SEND (McKean et al., 2025). Practitioners report the scripted questions can feel "alien" and unnatural, potentially confusing learners and impacting the reliability of their responses.
3. The Pressure of a Busy School
In practice, the one-to-one, time-intensive nature of the screening is a significant barrier. Studies have found that under severe time and staffing pressures, practitioners often compromise the standardised administration, using their "best judgement" to tick boxes rather than completing the full assessment (McKean et al., 2025). This fundamentally undermines the reliability of the data collected.
For SENCOs, the key takeaway is to treat WellComm as a valuable but imperfect screener. It is the start of an investigation into a learner's needs, not a definitive diagnosis.
How WellComm Compares to Other Language Screeners
WellComm is one of several popular language screening tools used in UK schools. Understanding the differences is key to choosing the right tool for your setting's needs.
Making WellComm Work in a Busy School: An Implementation Checklist
Effective implementation requires careful planning to mitigate the tool's limitations.
Planning Phase
[ ] Appoint a Lead: Designate one person (usually the SENCO) to be responsible for training, scheduling, and data oversight.
[ ] Schedule Protected Time: Block out assessment time in the school calendar. Trying to fit it in ad-hoc is a recipe for failure.
[ ] Find a Quiet Space: Identify a consistently available, quiet room for screenings. A corridor or noisy corner will invalidate the results.
[ ] Train Your Team: Ensure everyone administering the screen is trained not just on the 'how' but also the 'why' and the limitations.
Screening Phase
[ ] Follow the Script: Adhere to the standardised administration as closely as possible to ensure reliability.
[ ] Record Qualitative Notes: Don't just tick boxes. Note how the learner responds. Are they hesitant? Do they self-correct? This is rich data.
[ ] Be Mindful with EAL Learners: If screening an EAL learner, treat a Red or Amber score as an indicator of their current English language skills, not a sign of a disorder.
Action Planning Phase
[ ] Analyse by Need, Not Colour: Group learners by the type of language difficulty identified (e.g., understanding prepositions, verb tenses, vocabulary) rather than just their traffic light colour. This makes for more targeted groups.
[ ] Integrate, Don't Isolate: Use The Big Book of Ideas to inform your quality-first teaching. What language structures can be explicitly taught and practised in your upcoming science, history, or English lessons? For more on this, see The Importance of Oracy in Language Development.
[ ] Map Provision: Use the data to create a provision map that clearly shows which learners are receiving what support, and for how long.
Feature
WellComm Toolkit
LanguageScreen
Speech Link
Age Range
6 months - 11 years
3 years - 8 years
4 years - 8 years
What it Assesses
Receptive & expressive language (mainly vocabulary and concepts).
Receptive & expressive language.
Receptive language, speech sounds.
How it's Administered
One-to-one, paper-based, by a trained adult.
Online, adaptive, self-administered by the child with supervision.
One-to-one, administered by a trained adult using a laptop/tablet.
Key Strength
Provides a linked, comprehensive book of intervention activities. Covers a very wide age range.
Fast and efficient for whole-cohort screening. Highly engaging for learners.
Includes assessment of speech sound production, a key gap in other screeners.
Key Limitation
Time-intensive to administer. Criticised for low diagnostic accuracy and EAL/SEND suitability.
Intervention resources are less comprehensive than WellComm. Shorter age range.
More focused on speech sounds than broader language comprehension.
1. Can I use WellComm for EAL learners?
You can, but with significant caution. It is an assessment of English, not underlying ability. A low score for an early-stage EAL learner is expected and does not necessarily indicate a speech and language disorder. The data is best used to guide EAL support, not to diagnose SEND.
2. Is a WellComm report enough to refer to a Speech and Language Therapist?
No. An external therapist will conduct their own formal, diagnostic assessments. However, a WellComm report provides excellent evidence that the school has identified a need, put in a cycle of targeted support, and monitored the impact, which is a crucial part of the referral process.
3. How long does the screening take per child?
Allow for 15-20 minutes per child. For a class of 30, this represents a significant time commitment of around 10 hours. This must be factored into any implementation plan.
4. Can I just buy The Big Book of Ideas?
No, the two components are designed as an integrated system. The value of The Big Book of Ideas comes from its direct links to the assessment, allowing for targeted, data-driven intervention.
Your Next Step
Choose one specific language target from the WellComm 'Big Book of Ideas', such as understanding 'before' and 'after' or using regular plurals, and deliberately plan to teach and model it within one of your existing curriculum lessons next week. Observe which learners can use the language independently and which require more scaffolding. This small step will begin to shift your practice from isolated intervention to integrated, whole-class language support.
Research sources
Further reading from peer-reviewed research
These 5 studies give source context for the classroom guidance in this article on WellComm: using the speech and language toolkit well. They are included as starting points for deeper reading, not as a substitute for local professional judgement.
Screening for Speech and Language Delay and Disorders in Children 5 Years or Younger: Evidence Report and Systematic Review for the US Preventive Services Task Force.
C. Feltner et al. (2024) | JAMA
Translate the finding into explicit modelling, guided practice and progress monitoring rather than relying on one-off exposure.
Paul Main is an educator and metacognition researcher who founded Structural Learning in 2002. With a psychology degree from the University of Sunderland and 22+ years helping schools embed thinking skills, he bridges the gap between educational research and classroom practice. Fellow of the RSA and Chartered College of Teaching, with 128+ Google Scholar citations.