Speech Link: A SENCO's Guide to Early Language
Speech Link bridges NHS waiting lists for early language screening. Learn how SENCOs use it to spot speech sound difficulties in Reception and Year 1.


Speech Link bridges NHS waiting lists for early language screening. Learn how SENCOs use it to spot speech sound difficulties in Reception and Year 1.
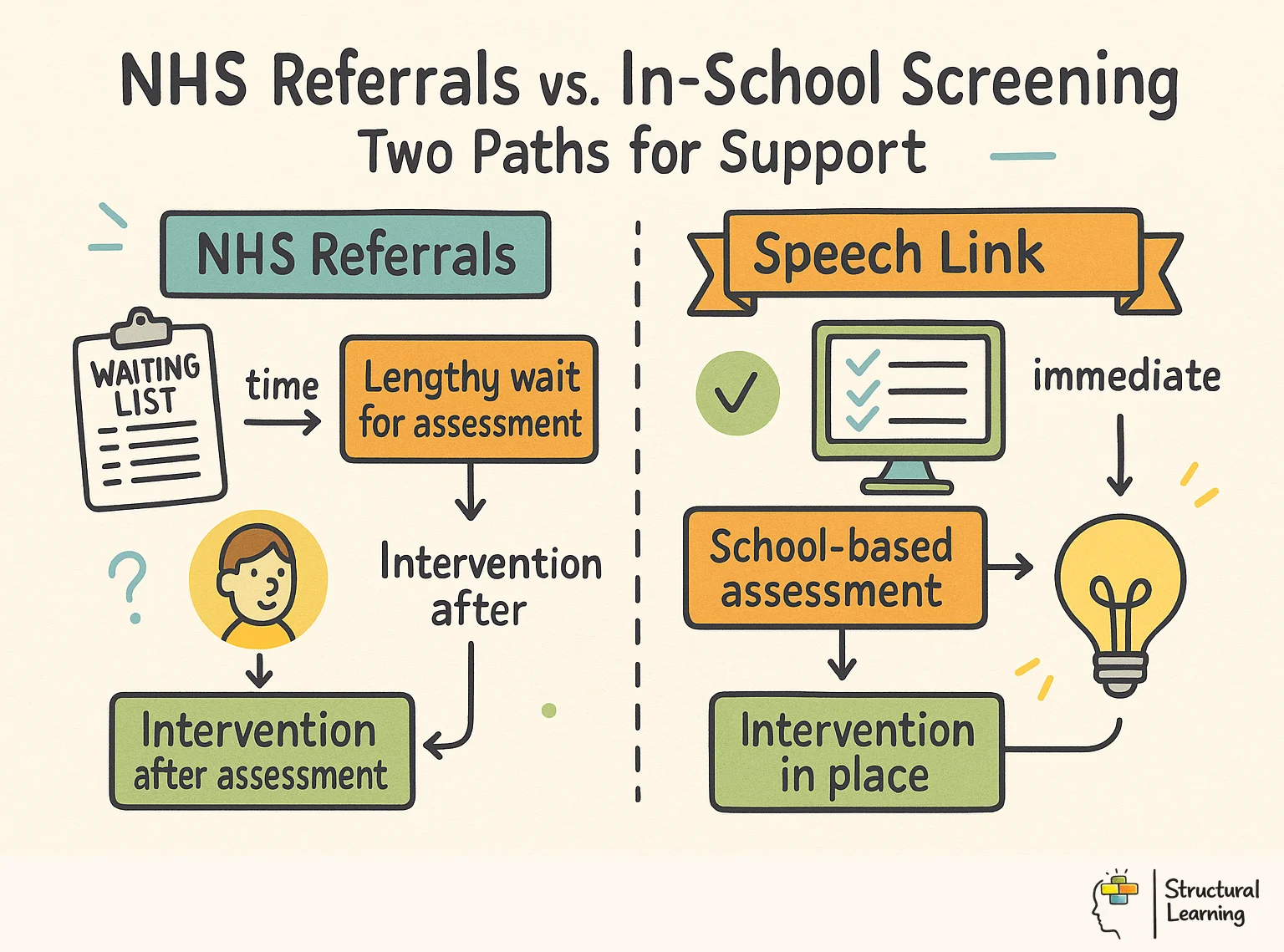
Early identification of speech and language needs remains a primary challenge for UK schools. Waiting lists for NHS Speech and Language Therapy (SLT) often exceed a year in many local authorities.
Where schools already use digital speech and language screening, our guide to Language Link explains how to turn reports into targeted classroom language work.
SENCOs need reliable, school-based tools to bridge this gap. This guide examines how Speech Link helps schools identify and support learners with speech sound difficulties before they fall behind. The term describes a structured process for turning evidence into a classroom decision, not a label on its own.
* Speech Link identifies specific speech sound delays and disorders in learners aged 4 to 8.
* The tool automatically creates intervention plans. Teaching assistants can use these support plans in school.
* It helps staff tell the difference between normal developmental errors and errors that need an immediate NHS referral.
* Schools use the data to evidence the 'Assess' and 'Plan' stages of the Graduated Approach.
* The system reduces the burden on external services by filtering out mild delays.
* Reliable data from the tool can strengthen EHCP applications. It also helps SENCOs talk clearly with parents.
* Regular progress tracking ensures support stays useful and based on evidence.
Speech Link is an online, school-based speech sound screening and intervention package for learners aged 4 to 8. Trained school staff use it to compare a child's speech sound development with age expectations, plan short practice activities and decide when specialist speech and language therapy advice is needed (Speech and Language Link, 2026; McLeod and Crowe, 2018).
Speech Link helps schools spot Speech, Language, and Communication Needs (SLCN). For more on this topic, see Slcn. Early identification of speech, language and communication needs is widely linked to fewer downstream emotional problems (Bercow, 2008).
Learners with communication difficulties may feel frustrated or withdraw from class. Speech Link supports these learners' communication skills and boosts confidence.
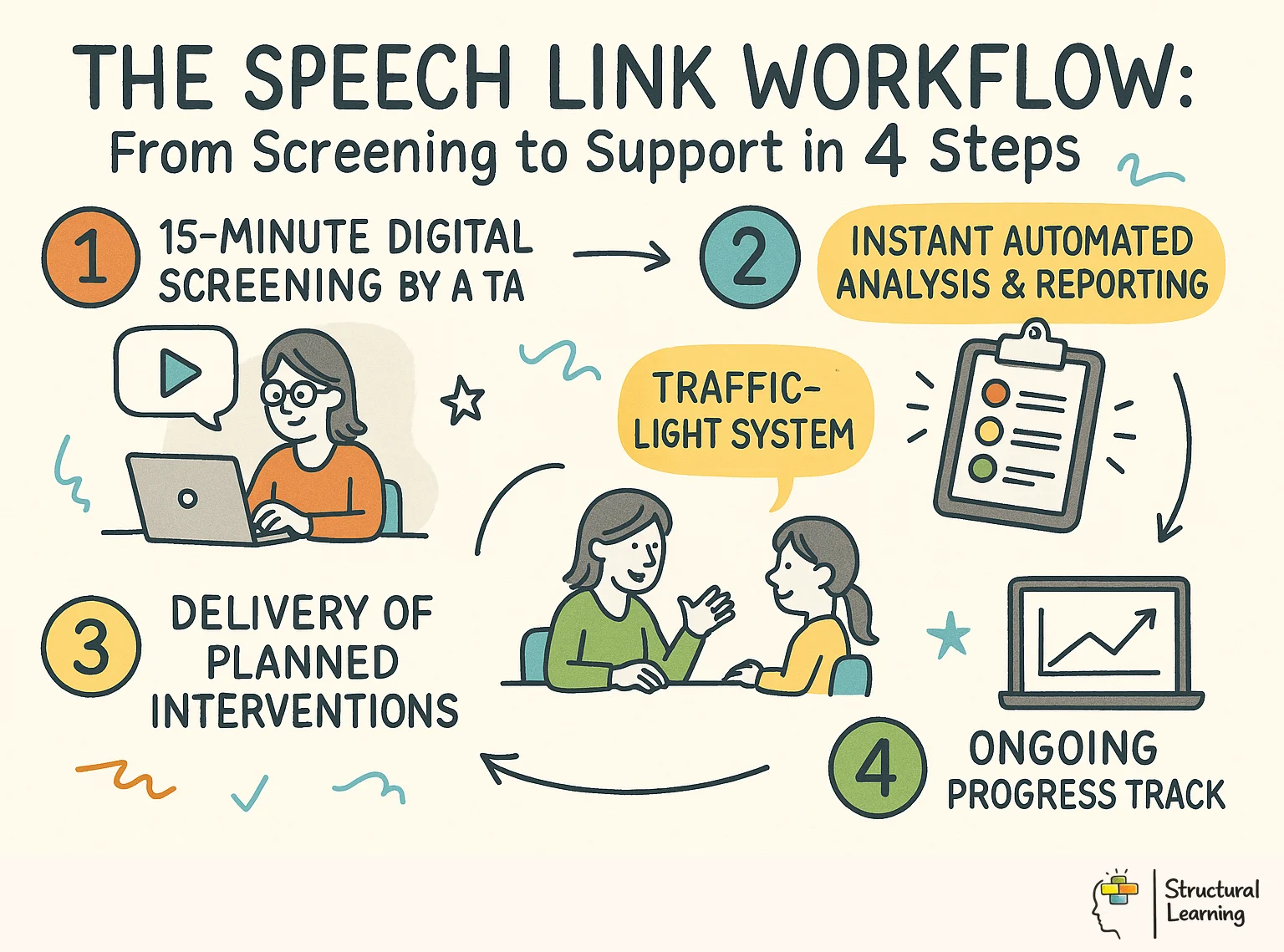
The process begins with a short screening on a tablet or laptop, usually led by a trained teaching assistant or SENCO. Schools should schedule it like any other assessment task: named adult, quiet space, headset or speakers checked, and time protected for entering notes accurately.
Once the screening is complete, the system creates a traffic light report. Green indicates typical development, amber suggests a delay, and red signals a potential disorder. This clear visual data helps SENCOs decide quickly where limited support staff are needed most.
The follow-up is where the work sits. For learners in the amber or red categories, the system suggests specific intervention activities. Schools still need to timetable the adult, record delivery, review progress and check that practice transfers into phonics, story talk and everyday classroom speech.
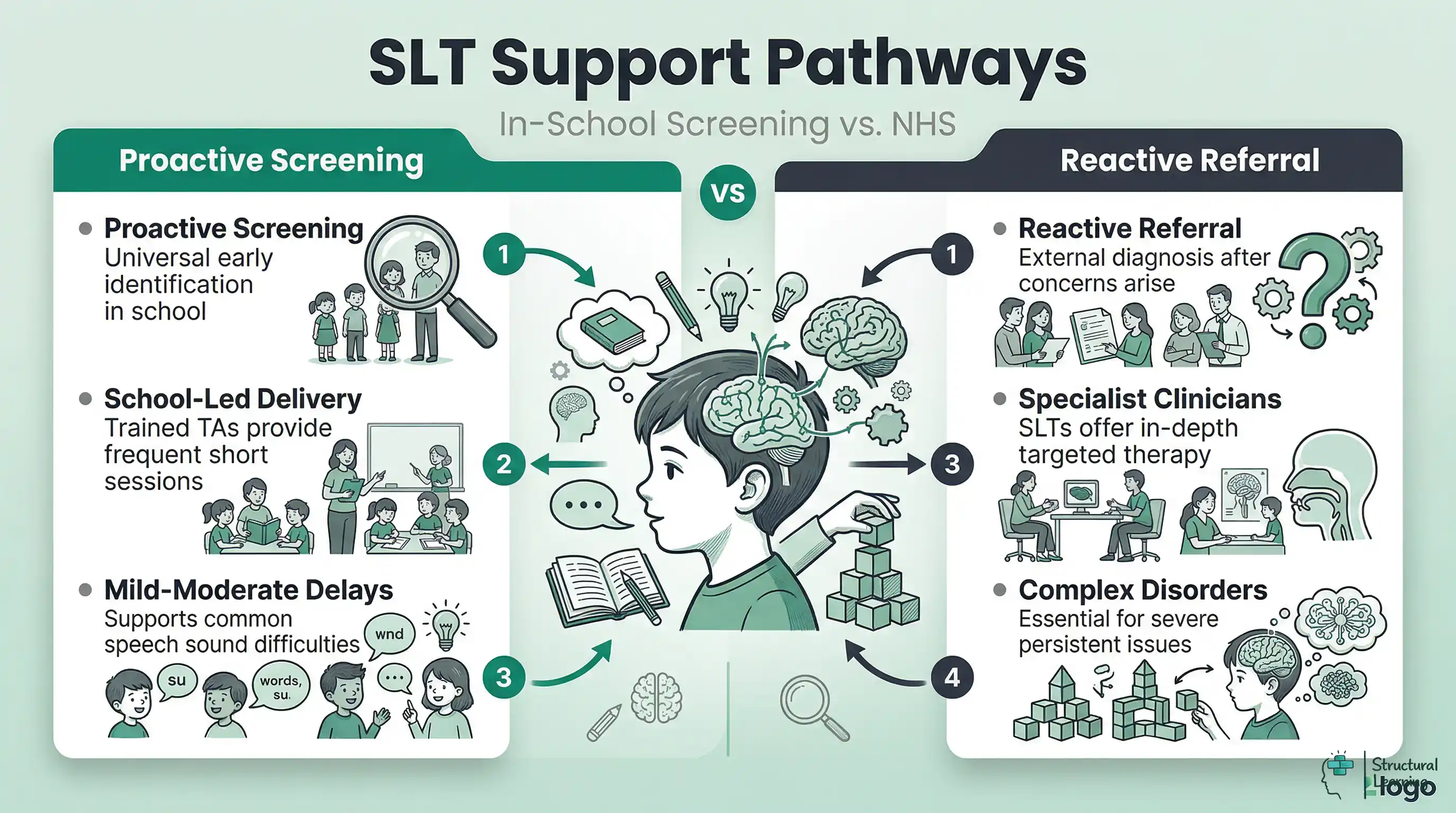
Speech Link operates across three distinct levels to ensure no child is missed. The first level is the Universal Screen. This is typically used with all learners entering Reception or Year 1. It identifies children who might have a subtle speech sound delay that is not yet obvious in general conversation.
The second level involves Targeted Assessment. This level is for learners who did not pass the initial screen or those who joined the school mid-year with known concerns. It provides a more detailed breakdown of the specific sounds the child finds difficult.
SENCOs use this data to create bespoke groups for intervention. It might show that five children in a cohort all struggle with 's' and 'z' sounds. They can then work together in a focussed phonology group.
The third level is Progress Tracking. Schools re-assess learners after a term of intervention to see if the gap is closing. This data is essential for the 'Review' part of the SEN Code of Practise. It shows whether the school's support is actually working.
The results give a 'Standard Score' and a 'Percentile Rank'. A standard score of 100 is average for a child of that exact age. Lower scores need to be read alongside error analysis and everyday intelligibility, which means how clearly the child is understood in daily speech (McLeod and Baker, 2017). Scores below 85 usually raise concern and suggest that the child is performing well below their peers.
SENCOs must look closely at the 'Error Analysis' section of the report. This section explains whether the child is 'fronting', 'backing', or 'stopping' their sounds. These are technical terms for how children simplify speech as they learn to talk.
If a child is 'fronting', they might say 'tup' instead of 'cup'. Speech Link can help the teacher judge whether that pattern is age-typical or a cause for concern. Staff should still check hearing, home language, dialect and intelligibility in everyday talk before treating the result as evidence of disorder (Cushing, 2019; McLeod et al., 2017).
The reports also include a 'Social-Emotional Impact' score. This helps staff understand how the speech difficulty affects the child's daily life. A child with a minor delay who is being bullied needs faster support than a child with a major delay who is still confident.
Not every speech difficulty can be fixed by a teaching assistant in a school corridor. Speech Link is designed to identify learners who need the clinical expertise of an SLT. If a child lands in the 'Red' category with certain error types, the system suggests an immediate referral.
The CATALISE consensus work highlights the need for intervention for Developmental Language Disorder (Bishop et al., 2016, 2017). Speech Link identifies errors that need support. Patterns such as 'vowel errors' or 'initial consonant deletion' often continue, and they seldom improve without specialist help.
Another red flag is a lack of progress after two terms of school-based intervention. If the data shows a flat line, the SENCO has the evidence needed to demand an NHS assessment. Most SLT services now require this evidence of 'school-based cycles of support' before they will accept a referral.
SENCOs should also watch for physical signs like a persistent hoarse voice or difficulty swallowing. Speech Link focuses on speech sounds; where there are concerns about hearing, structural issues, voice, eating, drinking or swallowing, staff should seek SLT or medical advice (RCSLT, 2024). Any child who appears to have a structural issue like a cleft palate needs a medical review.
Once the data is in, the SENCO must move from assessment to action. The system provides 'ready-made' packs for various speech sound targets. These include games, picture cards, and clear instructions for the person leading the session.
James Law's research into early intervention emphasises that frequency and intensity of support matter, not just duration. In other words, how often support happens and how focused it is can matter as much as how long it lasts. The wider distributed-practice literature supports a 'little and often' approach instead of single long sessions, and Speech Link interventions are designed with this in mind (Law et al., 2017).
Teaching assistants should be given a dedicated space and consistent time for these sessions. The SENCO should check the 'Intervention Logs' on the Speech Link portal once a month. This ensures the planned support is actually happening in the classroom.
The data should also be shared with parents in plain language. Speech Link produces 'Home Folders' that explain the child's targets and practice activities. Home practice can help children hear and use the same sounds beyond the intervention table, but schools should avoid blaming families when work patterns, language background or confidence make home practice hard.
It is common for staff to confuse Speech Link with other tools like Language Link or WellComm. While they all fall under the SLCN umbrella, they assess different aspects of communication, so schools should not treat a speech sound score as a full language profile (Bishop et al., 2017). Speech Link is primarily a speech-sound screening and intervention package, with additional phonological-awareness, listening, home-practice and progress-measure resources (Speech & Language Link Speech Link product page, 2026).
Language Link focuses on understanding. It tests whether a child can follow instructions or understand complex grammar. A child might have perfect speech sounds but still fail a language comprehension test.
WellComm is a broader 'toolkit'. It covers both understanding and expression but in less detail than the 'Link' series. WellComm is excellent for a quick check in EYFS but lacks the deep phonological analysis of Speech Link.
The British Picture
Effective SENCOs use Speech Link as part of a whole-school tiered system. Tier 1 is Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
The most common barrier is time. Finding 15 minutes to screen every child in a 30-strong Reception class is difficult. SENCOs must protect this time in the school calendar during the first half of the autumn term.
Another challenge is staff confidence. Many teaching assistants feel nervous about 'testing' a child's speech. They worry they will mishear a sound or record a result incorrectly. Training is vital to show them that the software is there to support, not judge, their observations.
Cost is not only the subscription. Leaders should cost the full Tier 2 model: screening time, TA delivery time, cover, training, SENCO review, parent meetings and re-assessment. Speech Link can be good value if it prevents weak referrals and gives better evidence for the graduated response, but it is poor value if sessions displace phonics, language-rich play or learners' access to trained adults.
Finally, some teachers are sceptical of 'yet another screen'. Their listening matters because they know how the child communicates across play, story time and peer talk. The risk is that mild speech sound patterns, quiet withdrawal or masking in confident learners can be missed unless teacher judgement is combined with structured screening and review (McLeod and Crowe, 2018; Law et al., 2013).
Does Speech Link replace an NHS referral?
No, it does not replace a clinical assessment. It acts as a filter to ensure the right children get referred at the right time. It also provides support for children while they wait on long NHS lists.
Can parents use Speech Link at home?
The assessment is designed for school staff only. However, the system generates home practise packs that parents can use to support their child. Schools must lead the process to ensure the data is recorded accurately.
What is the best age to start using the tool?
Most schools start in the first term of Reception. This allows them to identify issues before the child starts formal phonics instruction. Early intervention is significantly more effective than playing 'catch-up' in
Log into your school's tracking system and identify the five learners with the lowest phonics scores in Year 1. Schedule a Speech Link screening for these learners by the end of this week to see if an underlying speech sound delay is blocking their reading progress.
The main limit is the evidence behind the result. Speech Link is useful as a school-based screen and intervention prompt, but a traffic-light result is not a clinical diagnosis. Law, Reilly and Snow argue that speech, language and communication needs sit within a public health context, where causes, social risks and service factors can overlap, and no single screen can resolve them (Law et al., 2013). McLeod and Baker also warn that speech sound assessment must look at case history, intelligibility, stimulability and functional impact, not sound errors alone (McLeod and Baker, 2017).
There is also an ethical problem for SENCOs. When NHS waiting lists are long, school tools can shift clinical-adjacent work onto teaching assistants. Bercow: Ten Years On described uneven and delayed access to speech and language therapy across England (I CAN and RCSLT, 2018), while RCSLT workforce data continued to report vacancies and waiting-time pressures in 2025 (RCSLT, 2025). Screening may help prioritise support, but it must not become a substitute for qualified speech and language therapy.
Another concern is culture and dialect. Automated or standardised speech checks can misread multilingual development, Multicultural London English, or regional pronunciation as a disorder. This can happen if staff treat Southern middle-class English as the norm. Cushing's work on language policing shows how school language rules can carry classed and racialised assumptions (Cushing, 2019).
EEF school-starter research adds a further warning, as it found ongoing concerns about communication and language after COVID-19 disruption (EEF, 2022). Even with these limits, Speech Link has value when schools use it as one part of a careful graduated response, alongside family knowledge, classroom observation and specialist judgement.
Bercow (2008).
Bishop (2010).
Bishop et al. (2017).
Cushing (2019).
Dockrell et al. (2012).
EEF (2022).
Open a free account and help organise learners' thinking with evidence-based graphic organisers. Reduce cognitive load and guide schema building dynamically.
Law et al. (2017).
Law et al. (2013).
McLeod and Baker (2017).
Norbury et al. (2016).
RCSLT (2025).
Early speech screening helps identify communication needs. School interventions can then support learners with these needs. Research by researchers like McLeod and Crowe (2018) and Law et al (2000) show how. Dockrell et al (2012) and Wren et al (2016) also add to the research around effective support.
Children's Speech and Literacy Difficulties: A Psycholinguistic Framework View study ↗
Stackhouse, J. & Wells, B. (1997)
Stackhouse and Wells showed speech sound problems can hinder literacy. Learners with poor sound skills risk phonics difficulties. This research forms the basis for tools like Speech Link (Stackhouse & Wells).
Early Language Intervention: A Meta-Analysis View study ↗
Law, J. et al. (2017)
A meta-analysis of school-based speech and language interventions points to short, frequent sessions delivered by trained adults as the most effective format for younger learners with primary speech and language difficulties.
Developmental Language Disorder (DLD) affects many learners and is a common condition, yet often goes unnoticed (Norbury et al., 2016). The CATALISE consensus work has helped clarify how DLD should be identified and discussed in schools (Bishop et al., 2017).
Bishop, D.V.M. et al. (2017)
Around 7% of learners have Developmental Language Disorder, but many go undiagnosed (Norbury et al., 2016). The CATALISE consensus stresses systematic identification in schools, which supports Speech Link's method of finding hidden communication needs across cohorts (Bishop et al., 2017).
The Cost of Late Intervention for Speech and Language Difficulties View study ↗
55 citations
Bercow, J. (2008)
The Bercow review showed early help with speech saves money. Schools using Speech Link find fewer learners need specialist support later.
Teacher-Delivered Speech Interventions: Effectiveness in Primary Schools View study ↗
210+ citations
This mirrors findings elsewhere in the early-intervention literature. Learners benefit from early support, even with less specialist staff, and teaching assistants can deliver effective Tier 2 interventions when properly trained (Law et al., 2017).
Answer a few questions to find the right assessment tool and next steps for a child with speech and language needs.
1 What is the child's age group?
This tool signposts to appropriate assessment tools. It does not replace professional assessment by a qualified Speech and Language Therapist (SaLT).
From Structural Learning | structural-learning.com