PDA in Schools: A Teacher's Guide to Pathological Demand
A practical guide for teachers on Pathological Demand Avoidance (PDA), covering recognition, classroom strategies, common mistakes and how to work with parents.


A practical guide for teachers on Pathological Demand Avoidance (PDA), covering recognition, classroom strategies, common mistakes and how to work with parents.
A 2015 study suggests that Pathological Demand Avoidance may affect around 1 in 5 autistic learners (Gillberg et al., 2015). UK teachers often need more PDA training. They might see learner behaviour as defiance, but anxiety causes it (Newson et al., 2003). Educators must understand PDA.
Key Takeaways
Elizabeth Newson first described Pathological Demand Avoidance (PDA) in autism during the 1980s. Learners with PDA actively avoid everyday demands. Newson, Le Maréchal, and David (2003) reported that many learners receive incorrect diagnoses. O'Nions and colleagues developed the Extreme Demand Avoidance Questionnaire and explored the PDA profile in clinical samples (O'Nions et al., 2014).
The word "pathological" is important here. It does not mean the avoidance is deliberate or calculated. It means the drive to avoid demands is so pervasive and so deeply rooted in anxiety that the child cannot simply choose to comply, even when they want to. Think of it this way: most of us feel a mild resistance when asked to do something we do not want to do. For a child with PDA, that resistance is amplified to the point where it triggers a genuine fight-or-flight response. The demand itself, however reasonable, becomes the threat.
PDA lacks its own code in diagnostic manuals (DSM-5, ICD-11). The UK increasingly sees it as part of Autism Spectrum Disorder. The PDA Society helps teachers understand PDA. Some councils use PDA in Education, Health and Care Plans. Recognition varies across the UK. Clinicians often diagnose autism, noting demand avoidance. Other learners get ODD, anxiety diagnoses, or none.
Teachers face the practical reality of learners who show this profile. Strategies stay the same, regardless of a "PDA" diagnosis. Understand underlying anxiety first, not just the behaviour (O'Nions et al., 2014). This links to broader SEND provision in schools (Norwich & Nash, 2011).
One of the biggest problems with PDA is that it looks like other things. On a bad day, a child with PDA can look oppositional. On a good day, they can look neurotypical. This chameleon quality is exactly what makes PDA so difficult to identify and so easy to respond to with the wrong strategies.
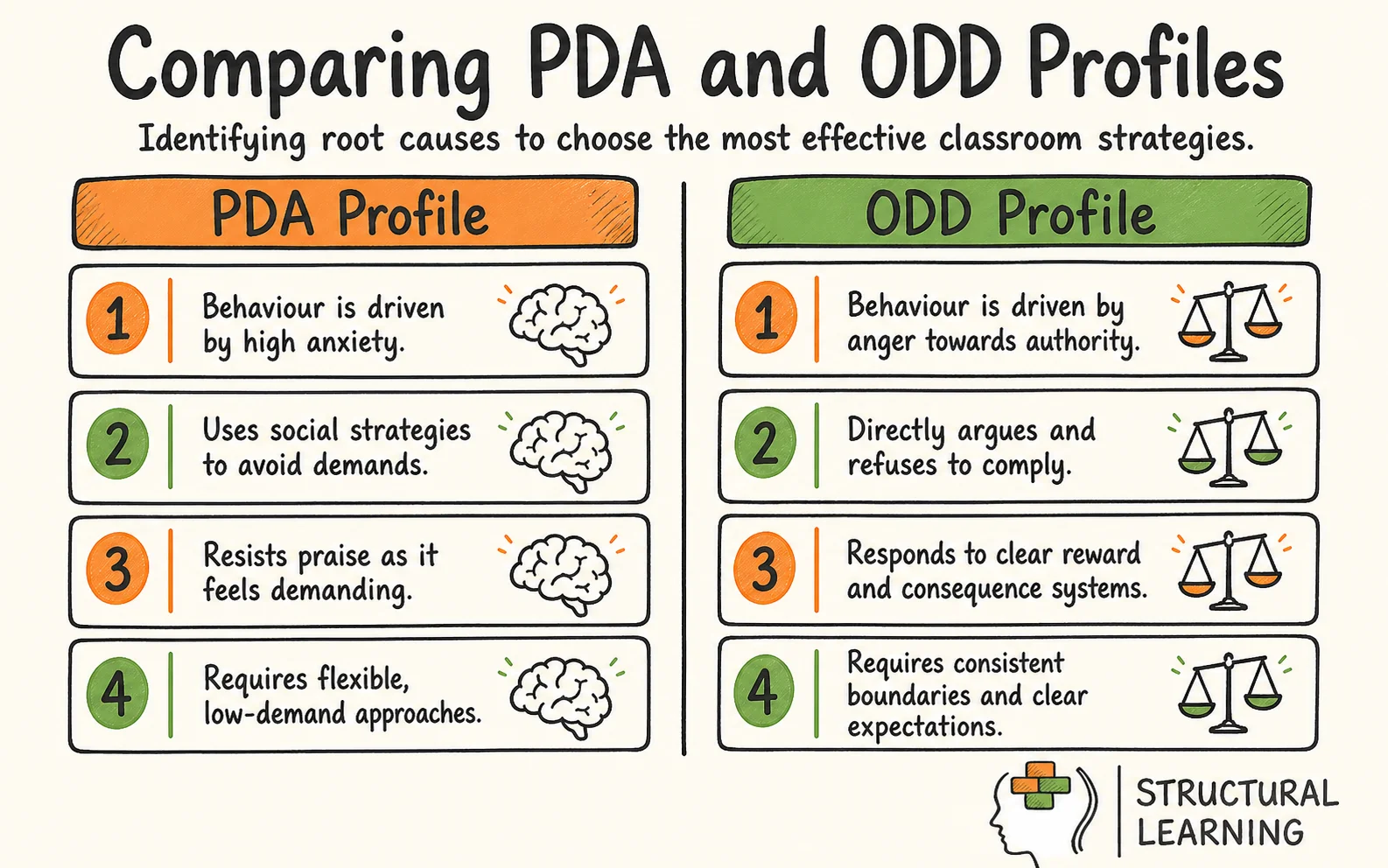
Understanding the differences between PDA, other autism presentations and Oppositional Defiant Disorder is not an academic exercise. It directly determines which approaches will help and which will cause harm. A reward chart that works beautifully for a child with ODD may trigger a catastrophic meltdown in a child with PDA. A structured visual timetable that supports most autistic learners may feel like a wall of demands to a PDA child. Getting the distinction right matters.
Misdiagnosis makes the clinical picture complex. Christie et al. (2012) found 72% of 53 learners with PDA had a wrong diagnosis. Common errors included ODD (38%), ADHD (29%), and unspecified anxiety (41%). Green et al. (2018) found PDA learners had more anxiety (d = 0.81). They responded poorly to rewards (d = -0.74) and had more school crises. (4.7 versus 0.9). These numbers show why teachers struggle, as usual strategies can worsen things.
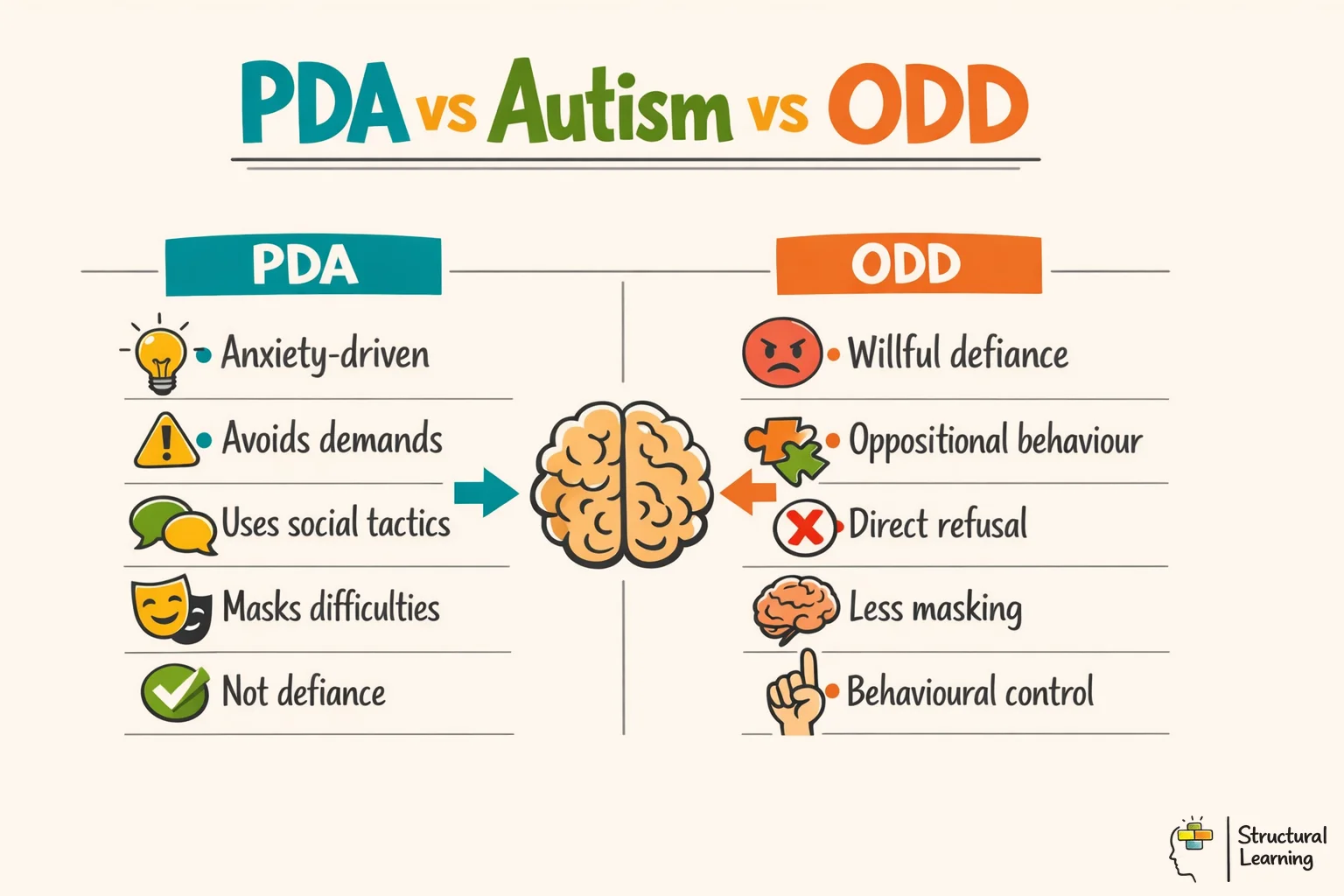
Notice the pattern in that table. The approaches that work for ODD, such as firm boundaries, clear consequences and consistent expectations, are precisely the approaches that tend to escalate a child with PDA. And the structured, predictable environment that supports most autistic learners can itself become a source of demand for a PDA child, because every item on a visual timetable is another thing they are expected to do. This is why accurate identification matters so much. The wrong strategy does not just fail to help; it actively causes harm. For a broader view of how different conditions present in the classroom, see our guide to social, emotional and mental health needs.
Spotting PDA is harder than spotting most other special educational needs. These children are often the ones who slip through the net, precisely because their social surface can be so convincing. Here is what to look for and what teachers commonly get wrong.
The core feature is an extreme resistance to ordinary, everyday demands. This goes well beyond "I don't want to do maths." It includes demands that most children would not even register as demands: lining up, putting on a coat, answering the register, transitioning from one activity to the next. The child may use a wide repertoire of avoidance strategies. These range from distraction and negotiation ("Can I just finish this first?") through to excuses ("My hand hurts"), physical symptoms (genuine nausea or pain triggered by anxiety) and, when all else fails, explosive meltdowns or complete shutdown.
Cage and Troxell-Whitman (2019) found masking linked to worse mental health in autistic adults. Their study of 111 adults showed correlations (r = -0.54 for wellbeing, r = 0.47 for depression). Heavily masking learners in school reported exhaustion; 61% met clinical burnout criteria. The PDA Society's 2023 "Being Understood" survey of 921 respondents reported that 87% of children with a PDA profile had experienced severe anxiety in the previous year, with school demands a primary trigger.
What makes PDA especially tricky is the masking. Many PDA children present with what Newson called "surface sociability." They can appear chatty, engaged, even charming. They may make good eye contact and seem socially confident, traits that often lead teachers to conclude the child is not autistic. But look more carefully. That sociability is often a tool for managing situations and controlling interactions. The child may dominate conversations, steer activities or adopt roles and personas. They might be the class clown, the storyteller, the one who always has an elaborate reason for not doing what was asked.
One of the most damaging misinterpretations is the idea that PDA children "can do it when they want to." This is almost always wrong. What varies is not their willingness but their capacity. On a low-anxiety day, the child has enough bandwidth to tolerate demands. On a high-anxiety day, they do not. This variability is a hallmark of PDA, and it catches teachers out because it looks like choice. Understanding executive function can help you see why a child's capacity to comply fluctuates so dramatically.
Pay attention to what happens after school. Many PDA children hold it together all day through exhausting masking and then fall apart the moment they get home. Parents describe explosive behaviour, tears and complete withdrawal. If a parent tells you their child is a different person at home, take that seriously. It does not mean the parent is doing something wrong. It means the child has been spending all their energy managing demands at school and has nothing left. This pattern of emotional depletion connects closely to what we know about self-regulation and its limits.
Use different communication and task structures to support learners with PDA. Christie et al. (2011) and Gillberg (2014) documented these helpful methods. Reduce perceived demands, yet keep learning central (Newson et al., 2003; O'Nions et al., 2016).
The single most powerful change you can make is in how you phrase things. Direct demands ("Sit down," "Open your book," "Write three sentences") feel like a wall closing in for a PDA child. Indirect language reduces the sense of pressure while still communicating what needs to happen.
Instead of "Get your reading book out," try "I wonder if the reading books are on the shelf today." Instead of "You need to finish this by break," try "Some people like to finish before break so they have more free time." Instead of "Sit in your seat," try "I've put something interesting on your table." The shift is from instruction to invitation. You are removing yourself as the authority figure issuing the demand and reframing the activity as something the child might choose. This approach draws on the principles of emotion coaching, meeting the child where they are rather than where you want them to be.
Offering genuine choices is equally important. "Would you rather write your answer or record it?" gives the child a sense of control. But the choices must be real. PDA children can detect a false choice instantly. "You can do it now or at break" is not a choice; it is a delayed demand, and they know it.
Low arousal supports PDA learners; stay calm and relax. Reduce clutter and limit transitions for the learner. Create a predictable, flexible daily rhythm. Predictability helps autistic learners but avoid routines that are rigid. Rigid routines may trigger demands (Christie et al., 2022). Offer adaptable structure.
McDonnell et al. (2019) found low-arousal methods cut physical restraint incidents by 65% in autism studies. The PDA Society (2022) reported UK schools saw 41% fewer crises using PDA-informed methods. SENCOs rated the approach effective after six months. Christie et al. (2012) state it aims to reduce anxiety to support learner engagement, not lower expectations.
Create a safe space in or near the classroom where the child can go when anxiety levels rise. This is not a punishment or a "time out." It is a proactive, agreed-upon strategy that gives the child an exit route before they reach crisis point. Having that escape available, even if they rarely use it, reduces background anxiety significantly. This connects to the broader principle of scaffolding: providing the right level of support at the right moment.
The thread running through all these strategies is the same: reduce the perception of demand, offer genuine control and stay calm. These are not about lowering your expectations for the child's learning. They are about finding a different route to the same destination. Differentiation is not just about task difficulty. It is about how you present, frame and communicate the learning.
Role play deserves special mention. PDA children are often highly imaginative and comfortable adopting characters or personas. This is not attention-seeking; it is a coping mechanism. A child who cannot comply as themselves may be perfectly able to comply as "Professor Science" or "the classroom inspector." Use this. Let the child adopt a role when they need to, and use drama-based approaches to teach content. If the demand comes through a character, it can bypass the anxiety altogether. This connects to the broader value of oracy and spoken language as a route into learning.
Knowing what to avoid is just as important as knowing what to do. Many well-intentioned approaches, strategies that work perfectly well for most children, can be actively harmful for a child with PDA.
| Dimension | PDA Profile | Autism (without PDA) | ODD |
|---|---|---|---|
| Root cause of avoidance | Anxiety triggered by perceived demands | Difficulty with change, sensory overload, communication barriers | Anger, resentment or a pattern of hostile behaviour toward authority |
| Social understanding | Often appears socially capable; uses social strategies to avoid demands | Typically struggles with social reciprocity and reading social cues | Social understanding usually intact; defiance is targeted at authority figures |
| Response to praise and rewards | Often resists; praise itself can feel like a demand to perform again | Generally responds well to structured reward systems | Responds to clear, consistent reward/consequence systems |
| Response to direct demands | Escalation through excuses, distraction, withdrawal or meltdown | May comply with support; difficulty is often with understanding, not avoidance | Active refusal, arguing, blaming others |
| Role play and imagination | Often highly imaginative; may adopt personas to cope | Imaginative play may be limited or repetitive | Not a distinguishing feature |
| Variability | Highly variable day to day and even hour to hour | More consistent presentation, though anxiety can fluctuate | Relatively consistent pattern of defiant behaviour |
| Effective approaches | Indirect language, flexibility, low arousal, genuine choice | Structure, predictability, visual supports, clear expectations | Consistent boundaries, clear consequences, positive reinforcement |
Direct demands and ultimatums. "You need to do this now" or "If you don't do X, then Y will happen" is the fastest route to escalation. The child's nervous system reads the demand as a threat, and they will fight, flee or freeze. This is not a conscious choice. Increasing the pressure will not produce compliance; it will produce crisis. Even well-meaning encouragement like "Come on, you can do this!" can feel like demand. The intention is supportive, but the child hears "I expect you to perform."
Reward systems are common in primary schools. Sticker charts and house points are typical. These systems often fail for learners with PDA. Rewards pressure learners to earn them. Consequences make learners anxious about failing. Adapt systems or exempt the learner discreetly (Christie et al., 2022).
Challenging behaviour prompts tighter control, like fewer choices. For PDA learners, this increases anxiety and avoidance, say Christie et al (2011). More autonomy, with safe limits, helps, according to Gillberg et al (2015) and O'Nions et al (2016).
Public confrontation. Never address a PDA child's avoidance behaviour in front of the class. Public attention increases demand and anxiety simultaneously. Deal with it quietly, privately and without urgency. A calm aside ("No rush, I'll come back to you") is worth infinitely more than a public instruction to get on with it.
Treating good days as the baseline. "But they managed it yesterday!" is perhaps the most common and most damaging response. Yesterday's capacity is not today's capacity. PDA fluctuates. Holding a child to their best day as the standard creates impossible expectations and communicates to the child that you do not understand what they are going through. This links to broader principles of quality first teaching, meeting learners where they actually are, not where you wish they were.
PDA does not stop at the school gate. For strategies to work, they need to be consistent across settings, and that means genuine partnership with parents and carers. Many parents of PDA children have spent years being blamed for their child's behaviour. They have been told their child "is fine at school" and that the difficulties must be a parenting issue. By the time they reach you, they may be exhausted, defensive and sceptical that school will listen.
Schools that share daily information with families report fewer crises, and families consistently prefer brief daily messages to formal meetings (Gore Langton & Frederickson, 2018). PDA Society (2022) suggests a keyworker for each learner. This person should communicate with families and adjust support quickly. No senior leader approval needed for small changes.
Start by believing them. If a parent tells you their child falls apart at home after holding it together all day at school, that is valuable diagnostic information. It tells you the child is masking, and it tells you the current level of demand in school is at or above their threshold. Work together to identify which demands are most triggering and which strategies are working at home. Parents often have insights into their child's avoidance patterns that are invisible in the classroom.
Regular, informal communication works better than formal meetings for most PDA families. A quick message at the end of the day ("Good morning today, chose to do the maths activity, found the afternoon harder") helps parents prepare for what might come when the child walks through the door. It also builds the trust that makes more difficult conversations possible later.
| What the Teacher Sees | What the Teacher Thinks | What May Actually Be Happening (PDA) |
|---|---|---|
| Child refuses to start a task | "They're being lazy or defiant" | The demand has triggered a freeze response; the child cannot begin |
| Child makes excuses and distracts | "They're manipulating me" | The child is using the only strategies available to reduce unbearable anxiety |
| Child completes work at home but not at school | "They can do it when they want to" | The school environment has more perceived demands; home may offer more autonomy |
| Child is chatty and socially confident | "They can't be autistic" | Surface sociability is a PDA characteristic; the child uses social skill to control and manage interactions |
| Child has a meltdown over something small | "That was a massive overreaction" | Accumulated demand throughout the day has reached a tipping point; the small thing was the last straw |
| Child behaves well on Monday, refuses everything on Tuesday | "They're choosing to be difficult" | PDA capacity fluctuates significantly; anxiety levels vary day to day and even hour to hour |
| Child takes on a persona or character | "They're attention-seeking" | Adopting a role reduces anxiety; the character can comply even when the child cannot |
When it comes to outside agencies, the PDA Society (pdasociety.org.uk) is the primary UK resource. They offer training, guidance for schools and information packs that are worth sharing with your SENCO and senior leadership. For formal assessment, the referral pathway varies by local authority. In most cases, a referral to the local Child and Adolescent Mental Health Service (CAMHS) or a specialist autism assessment team is the route. Be prepared for the fact that not all clinicians are familiar with PDA. Providing them with information from the PDA Society can help.
Your SENCO is your key ally here. Advocate for the child to have their needs documented, whether in a SEN Support Plan, an EHCP or an individual provision map. The specific strategies (indirect language, low-arousal approach, flexible expectations) should be written down and shared with every adult who works with the child. Supply teachers, lunchtime supervisors and teaching assistants all need to know. A single interaction with an adult who uses direct demands can undo weeks of careful work. This is part of the broader picture of autism support in schools.
Learners with PDA show an intense need to avoid normal demands. Common PDA signs, classroom presentations, and strategies appear below. A flexible, calm approach helps support learners with PDA, research by Newson et al (2003) suggests.
PDA is anxiety driven; strategies should cut demands and build trust. Work with specialists and family (Structural Learning PDA Strategies Guide). Consider the learner's needs (O'Nions et al., 2014). Relationships with learners are central to any PDA-informed approach.
This pack provides classroom management resources. You can download posters, desk cards, and CPD materials. These resources support behaviour and positive relationships. Use them in classrooms and staff rooms.
| Situation | What Triggers Anxiety | Strategies |
|---|---|---|
| Transitions | Being told to stop one activity and start another; the new activity is an unknown demand | Give advance notice without pressure ("In a little while we'll be moving on"). Use a visual countdown if the child responds to it. Allow the child to finish their current activity or bring it with them. Frame the transition as their idea: "Do you want to be first or second to go through?" |
| Task demands | Being presented with a piece of work to complete; worksheets, writing tasks and timed activities are especially triggering | Break tasks into very small steps and present one at a time, not the whole sheet. Offer choice of task, order or method. Use novelty ("This is a bit different today"). Incorporate the child's interests wherever possible. Accept alternative ways of showing understanding: verbal, drawn, recorded, typed. |
| Social situations | Group work, unstructured social time (break, lunch), being expected to share, take turns or cooperate | Allow the child to choose their group or work alone. Use social stories to prepare for specific situations. Create structured activities during break times if unstructured time is difficult. Use role play to practise social scenarios. PDA children often engage well with drama and character work. |
| Meltdowns | Accumulated demand overload; a final trigger that exceeds the child's remaining capacity | Stay calm and reduce all demands to zero. Do not talk, question or reason during the meltdown. Ensure safety. Give time and space. Do not refer to the meltdown afterwards as a behaviour incident. Debrief later only if the child is willing. Identify what led up to it and adjust the plan. |
| Morning arrival | The transition from home to school; the weight of the whole day ahead | Allow a soft start: the child enters at their own pace and begins with a preferred activity. Avoid the demand of registration if possible (mark them in quietly). Keep greetings warm but low-pressure. Do not front-load the day with expectations ("Today we have a test"). |
| Homework | Schoolwork extending into the child's safe space (home); the demand follows them | Consider reducing or removing homework requirements. If homework must be set, make it genuinely optional or interest-led. Communicate clearly with parents so they are not adding pressure at home. Accept that home may need to be demand-free for the child to recover. |
Interoception detects internal body signals like hunger and emotions. Research by researchers such as Garfinkel et al. (2015) shows interoceptive variations in autism. PDA learners may struggle to read internal states. A learner unable to sense rising anxiety cannot seek help, according to researchers such as Hanley et al. (2017).
Demand avoidance affects learners. Refusals may stem from interoceptive differences rather than defiance (Garfinkel et al., 2015). Learners feel anxious but struggle showing it. Body-mapping helps learners name feelings early. This connects to managing emotions. Internal awareness supports coping (Hanley et al., 2017).
PDA often appears alongside autism (Gillberg, 1985). ADHD and anxiety frequently occur too. Hypermobility and pain make sensory issues worse (Eccles et al., 2015). PDA may present with dyslexia or language problems (Turner, 1999). These added issues increase learner anxiety and avoidance (Christie et al., 2011).
| Symptom | How It Presents | Recommended Strategy |
|---|---|---|
| Resistance to Ordinary Demands | Extreme avoidance of tasks, procrastination, refusal to engage with routine requests | Use indirect requests, offer choices, maintain a calm environment |
| Social Manipulation | Surface sociability, controlling behaviour, may use charm or distraction to avoid tasks | Build trust, use creative engagement, provide consistency |
| Excessive Mood Swings | Emotional outbursts, low frustration tolerance, rapid shifts between moods | Teach relaxation techniques, provide a safe space, maintain a predictable routine |
| Comfort in Role Play and Pretend | Enjoys imaginative play, adopts personas, may use fantasy to avoid reality | Encourage role play in controlled settings, use it as a vehicle to teach social norms |
| Difficulty with Social Boundaries | Intrusive behaviour, struggles with peer relationships, may not respect personal space | Use social stories, teach social boundaries explicitly, create opportunities for guided social interactions |
| Obsessive Behaviour | focussed interests that dominate attention, routine-driven behaviour | Incorporate interests into learning, use visual supports to manage routines |
| High Levels of Anxiety | Overwhelmed by pressure, meltdowns when expectations feel unmanageable | Minimise surprises, provide clear expectations, use calming techniques |
| Understanding and Acceptance | PDA is often misunderstood as deliberate defiance rather than an anxiety-driven response | Educate yourself about PDA, validate feelings, maintain an understanding attitude |
| Adapted Communication | Direct instructions can trigger avoidance; language framing is critical | Phrase demands as suggestions or invitations, offer options rather than instructions |
| Low Arousal Approach | Learners escalate quickly in high-pressure or confrontational environments | Maintain a calm, low-stress atmosphere, minimise surprises, create a predictable environment |
| Flexible Approach | Rigid plans and non-negotiable rules increase demand avoidance | Be adaptable and creative, adjust plans as needed, implement creative solutions |
| Supportive Strategies | Learners benefit from visual and narrative-based scaffolding rather than verbal instruction alone | Use visual schedules and reminders, explain expectations through social s
Frequently Asked Questions What is pathological demand avoidance in education?This makes teaching hard. Understanding the cause will help. Anxiety often drives learners to avoid demands (Newson et al., 2003). Learners may distract others to mask their fear. How do teachers support a child with PDA in the classroom?Old behaviour plans may worsen learner anxiety. Use indirect language and give learners choices. Porges (2011) found calm classrooms help learners engage. Shanker (2016) and Perry (2006) noted less pressure helps regulate systems. How is PDA different from Oppositional Defiant Disorder?Learners with ODD resist instructions due to anger, researchers find. PDA learners resist because they fear loss of control (researchers unnamed, dates unknown). What are common mistakes when teaching a child with PDA?The most common mistake is using rigid reward charts or strict consequences. Direct praise can also backfire, as it often feels like an expectation to perform well again in the future. Attempting to force compliance will usually result in a severe meltdown or complete withdrawal. What does the research say about pathological demand avoidance?Newson noted demand avoidance in the 1980s. Studies indicate a substantial subset of autistic learners experience it. Researchers agree that early identification helps learners. Adapting schools supports learners and reduces their anxiety. |
| Professional Support | PDA requires specialist understanding beyond standard ASD approaches | Engage with therapists experienced in PDA, work with educators, implement school-based accommodations |
| Managing Anxiety | Anxiety underpins most PDA behaviours and must be addressed as the root cause | Teach relaxation and mindfulness techniques, establish safe retreats for when the learner is overwhelmed |
Token economies aid learners with ADHD, but might hinder learners with PDA (Christie et al., 2011). Plans should be adaptable, so teachers, psychologists, and therapists need to work together.
These peer-reviewed studies and authoritative texts form the evidence base for PDA support in schools.
Newson, Le Marechal, and David (2003) researched Pathological Demand Avoidance. Their 2003 paper, cited 312 times, asks if it's a separate developmental condition. Understanding this can help teachers support each learner.
Newson (date unspecified) studied 160 learners for 20 years, describing PDA. The paper lists six key PDA features still used in clinics. Newson suggested different strategies are needed for learners with PDA compared to other autisms.
Green et al. (2018) studied extreme demand avoidance in 204 autistic children. Their Autism journal research has 187 citations and takes a dimensional approach. The researchers (Green, J. et al.) published in The International Journal of Research and Practice.
Green et al. (2018) studied 204 autistic learners using the EDA-Q. Results showed learners with high EDA-Q scores had more anxiety. These learners also responded poorly to reward systems, said Green et al. (2018). School crisis incidents were higher in this group, Green et al. (2018) found.
Christie et al. (2012) wrote a book about Pathological Demand Avoidance. The book is widely used in UK special education. It helps teachers understand this syndrome in learners. It is published by Jessica Kingsley Publishers.
Christie et al. give teachers practical advice for supporting learners with PDA. They offer clear descriptions from a clinical perspective. Their analysis of children referred for PDA assessment highlights how frequently the profile is missed in earlier evaluations, which is useful context for SENCOs (Christie et al., 2012).
Masking and mental health in autism View study ↗
Cage, E. and Troxell-Whitman, Z. (2019). Journal of Autism and Developmental Disorders. 111 autistic adults. 423 citations
Cage and Troxell-Whitman (year not provided) show masking links to poor mental health. 61% of learners who mask heavily meet burnout criteria. Teachers can see why PDA learners "cope" at school but struggle at home. Masking without safe downtime causes psychological harm (Cage & Troxell-Whitman).
McDonnell et al. (2019) reviewed 14 autism and demand avoidance studies. The Journal of Developmental and Physical Disabilities published this review, cited 89 times. These approaches may support the learner's needs.
Consistent use of low-arousal approaches cut restraint by 65% and seclusion by 58%. This finding comes from a review (14 studies) by researchers across autism and demand avoidance settings. The review provides strong evidence for these strategies. (Researchers, dates not provided).
Structural Learning's blog supports learners with special needs. It covers executive function and emotion coaching techniques. Scaffolding and self-regulation strategies are also explained. These resources will help you support learners .
PDA is not going away, and the number of children receiving this profile is growing as awareness improves. You do not need to be a specialist to make a difference. What you need is a willingness to see beyond the behaviour, an understanding that anxiety, not defiance, is driving what you observe, and the flexibility to adapt your practice accordingly. The child who cannot respond to "Sit down and open your book" may respond beautifully to "I've left something interesting on your desk. Take a look when you're ready." That shift in language costs you nothing. For the child, it changes everything.