Oppositional Defiant Disorder: A Classroom Guide
A practical guide to recognising and supporting learners with Oppositional Defiant Disorder, using evidence-based strategies and a consistent support plan.


A practical guide to recognising and supporting learners with Oppositional Defiant Disorder, using evidence-based strategies and a consistent support plan.
Every school in the UK has learners who push back against rules, argue with adults and seem to resist authority at every turn. For most children, this is a passing phase. But for the small but significant proportion of school-age children in the UK who meet the criteria for Oppositional Defiant Disorder (ODD), the pattern runs deeper, lasts longer and disrupts learning for the child and their classmates alike. If you are a teacher, teaching assistant or SENCo, understanding ODD is not optional. It is a core part of your professional toolkit for special educational needs provision.
ODD is common but often misunderstood, say many teachers. They may see learners as deliberately misbehaving. ODD is a clinical condition with diagnostic rules (researchers disagree). These learners need structured support focused on relationships rather than just punishment.
The DSM-5 defines ODD as a six-month pattern of anger, defiance, and revenge seeking. These behaviours, aimed beyond siblings, exceed typical age expectations. Remember, all learners argue sometimes. ODD diagnosis requires persistent behaviours that significantly impair social, educational, or family life.
ODD usually starts before age eight, but can develop later. Studies show early onset links to lasting problems (Journal of Child Psychology and Psychiatry). Boys are diagnosed more often than girls when young. This gap lessens in teens, possibly due to referral bias, not actual differences.
DSM-5 groups ODD symptoms in three areas. These are: angry mood, defiant behaviour, and vindictiveness. Learners need four symptoms total (APA, 2013). Vindictiveness needs two instances in six months (APA, 2013).
Research shows ODD describes behaviour patterns, not causes. (Hinshaw & Anderson, 2022). Temperament (Barkley, 1997), family environment (Patterson, 1982), and biological differences affect learners. Executive function and emotional regulation are also implicated (Diamond, 2013).
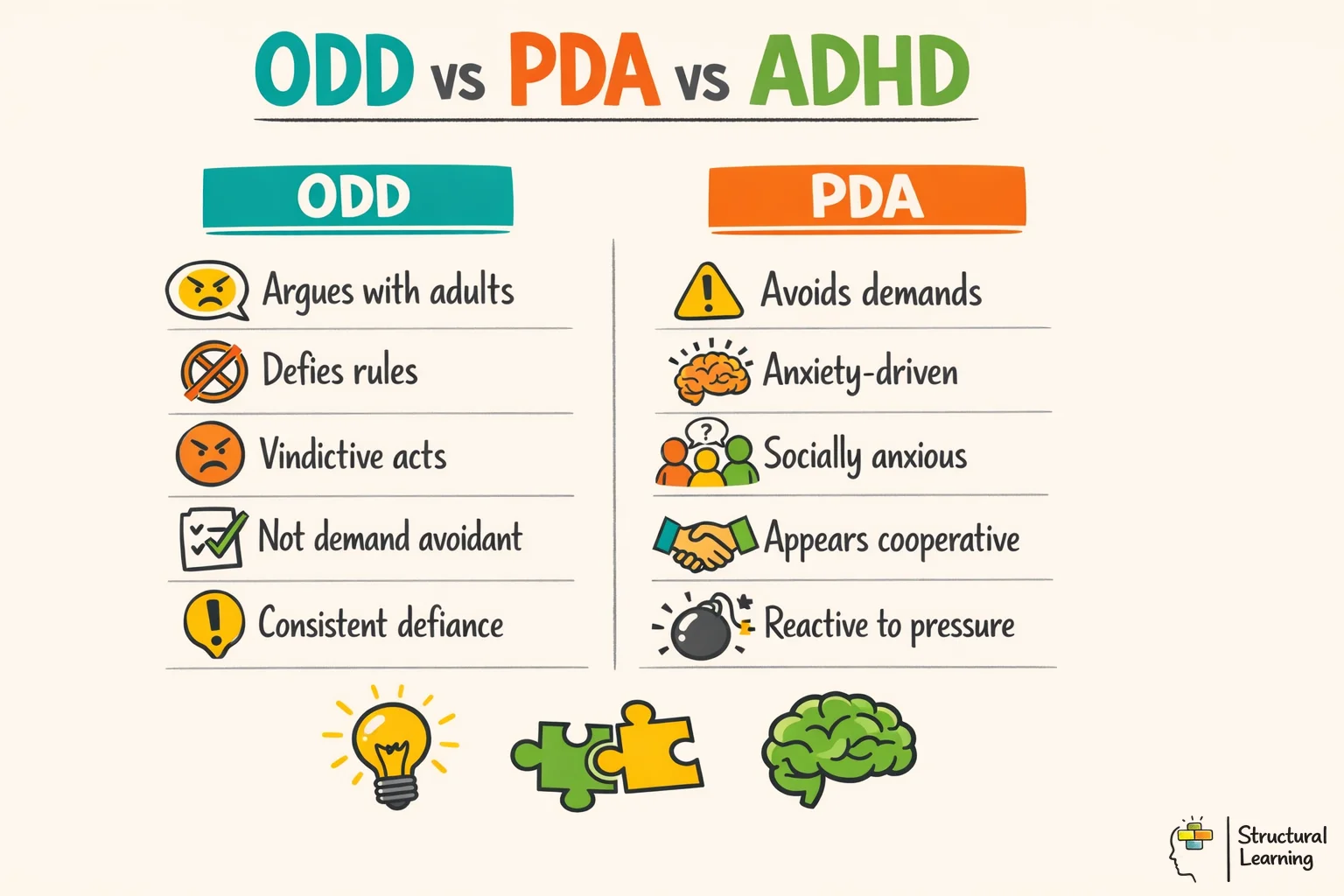
One of the most common mistakes in schools is treating all oppositional behaviour as if it has the same cause. A learner with Pathological Demand Avoidance (PDA), a profile of autism, may look similar to a learner with ODD on the surface. Both refuse adult requests and resist rules. But the underlying drivers are entirely different, and strategies that work for one group can backfire badly with the other.
ADHD and ODD often occur together. Research consistently shows that a substantial proportion of learners with ADHD also meet criteria for ODD, with some studies reporting comorbidity rates of around 50% (Johnston et al., 2003). Schools may misinterpret undiagnosed ADHD as defiance, missing executive function challenges. Conduct Disorder (CD) features more severe antisocial actions. These include aggression, vandalism, and deceit. ODD can precede CD, yet they remain separate conditions.
Oppositional Defiant Disorder shows as lasting anger and arguments. Learners often argue with adults and defy requests (APA, 2013). Prevalence estimates vary, with a 2018 NHS report finding 2.9% of children in England met criteria for ODD. Structured support manages this condition better than punishment (Kazdin, 2005).
Proactive strategies work better than reacting to difficult behaviour. Consistent routines, clear expectations, and positive reinforcement reduce confrontation. Give calm instructions, avoid power struggles, and offer choices with known consequences (Researchers, Dates).
Teachers often assume all oppositional behaviour stems from the same cause. They may mistake ODD for PDA or ADHD, needing varied responses. Demands help some with ODD, but can cause anxiety for a learner with PDA.
ADHD and ODD often occur together, with rates reaching 60%. Schools may misinterpret defiant behaviours from learners (Johnston et al., 2003). Overlooking executive function deficits hinders proper support (Barkley, 1997). Diagnosing both conditions enables better learning plans.
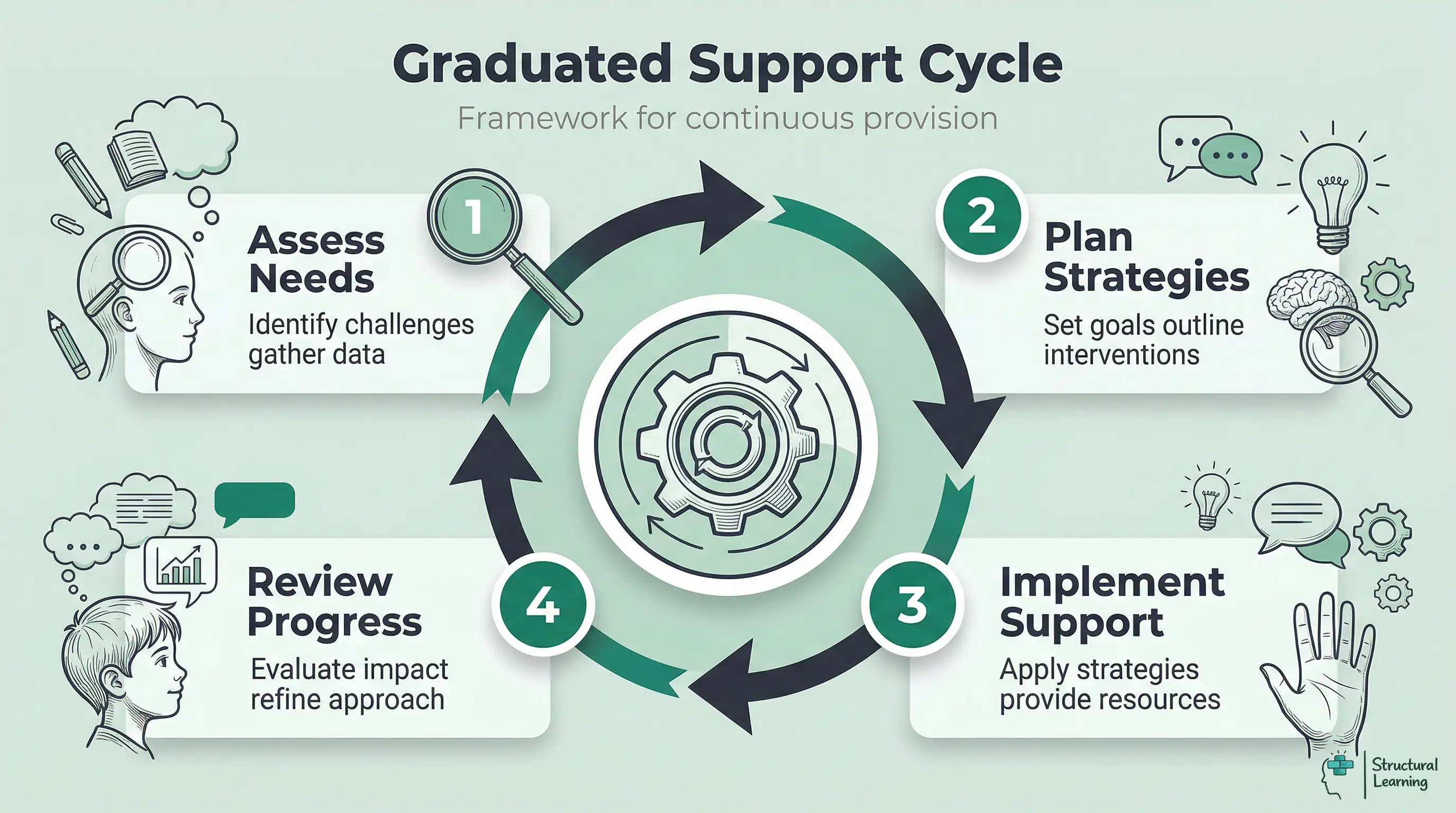
Assess, Plan, Do, Review gives schools structure for progress tracking. It stops staff relying only on instinct with difficult behaviour (Assess, Plan, Do, Review). This method ensures interventions adjust based on evidence. Classrooms are calmer, and learners achieve better results using this approach (Assess, Plan, Do, Review).
Why does this matter for classroom practice? Because a PDA learner who is given a firm, direct instruction ("You need to sit down now") is likely to experience a surge of anxiety that makes compliance harder. The same instruction may be exactly the right approach for a learner with ODD, provided it is delivered calmly and paired with a known consequence. Getting the identification right is the first step towards getting the strategy right. If you are unsure, consult your SENCo and consider a referral for a multi-disciplinary assessment.
What does ODD actually look like in a primary or secondary classroom? It is rarely the dramatic, table-flipping image that comes to mind. More often, it is a persistent, low-level pattern that wears teachers down over weeks and months. The learner who argues with every instruction. The child who refuses to start work unless conditions are exactly right. The young person who blames everyone else when things go wrong. These patterns, taken individually, look like ordinary misbehaviour. Taken together, over time, they form a recognisable clinical picture.
This table helps you spot learners who may need extra support. It uses DSM-5 criteria adapted for the classroom. You can use it to identify behaviours that warrant further review.
Do not diagnose ODD; clinicians do that. Recognise patterns, document them, and refer learners (Barkley, 2006). Consider other causes for behaviour (Prior & Glaser, 2006). Bereavement, learning needs, or self-regulation may explain it. Remember, context is very important (Vygotsky, 1978).
Talk to your SENCo about behaviour patterns over six months that badly affect a learner’s progress or friendships. Bring records with frequency data, examples, triggers and used strategies. Documentation links classroom observations to clinical assessments.
Punishment worsens ODD, research shows. Proactive management, de-escalation plans and clear limits are key. Build relationships with learners. This helps reduce oppositional behaviour intensity and frequency. Teach learners better emotional regulation skills (Kazdin, 2017).
Learners with ODD need consistent strategies, as noted by researchers (e.g., Barkley, 2006). Some tactics resemble general behaviour management. However, learners with ODD need systematic, unwavering application (Webster-Stratton, 2005; Patterson, 1982).
Notice the common thread running through every strategy: you stay calm, you stay consistent and you avoid getting drawn into the power struggle. This is emotion coaching in practice. You acknowledge the child's feelings while holding firm on expectations. It is harder than it sounds, especially on a Friday afternoon in a class of 30. But it works.
These strategies support quality teaching. Clear instructions and routines help every learner. Differentiated expectations and good relationships are key. These steps are vital for learners with ODD. Reducing triggers prevents confrontation (researchers/dates not included).
Understanding what not to do is just as important as knowing what to do. Some of the most instinctive responses to oppositional behaviour are precisely the ones that make it worse. If you have ever found yourself in a ten-minute standoff with a learner while the rest of the class watches, you already know how this feels.
| Feature | ODD | PDA (Autism Profile) | ADHD | Conduct Disorder |
|---|---|---|---|---|
| Primary driver | Anger, defiance towards authority | Anxiety-driven demand avoidance | Impulsivity, inattention | Aggression, rule violation |
| Response to direct demands | Argues, refuses, escalates | Panics, withdraws, uses distraction or social strategies to avoid | Forgets, gets distracted, loses focus | Ignores or intimidates |
| Empathy and remorse | Usually present after calming | Usually present but masked by anxiety | Usually present | Often reduced or absent |
| Typical onset | Before age 8 | Early childhood | Before age 12 | Childhood or adolescence |
| Social relationships | Conflict with authority; peers may be fine | Difficulties reading social cues; may mask | Often wants friendships but struggles with impulse control | May use relationships instrumentally |
| Effective approach | Consistent boundaries + positive relationship | Reduced demands, flexibility, indirect language | Structure, prompts, movement breaks, medication review | Multi-agency, specialist intervention |
Power struggles. This is the number one trap. A learner with ODD will argue with you for as long as you are willing to argue back. Every exchange raises the emotional temperature and deepens the confrontation. The moment you engage in a back-and-forth debate about whether a rule is fair, you have already lost the battle. State the expectation. State the consequence. Walk away. Return in two minutes.
Correcting a learner with ODD publicly will likely make things worse. Learners feel humiliated, which triggers defiance (Barkley, 2006). Whenever possible, speak quietly at their desk. Alternatively, move conversations to the corridor or use a private signal.
Consistent rules are key. Learners see defiance as sensible if consequences change (Alberto & Troutman, 2013). Why obey if rules are sometimes ignored? All adults must use the same strategies. This includes all staff (Lewis & Sugai, 1999). Use one-page profiles and behaviour plans for clarity. (Kern & Clemens, 2007).
Zero-tolerance rules often fail learners with ODD; these need relationship-based strategies. A blanket "three strikes" rule may suit most learners. But for learners with ODD, it can break relationships. Tailor behaviour management as you would learning (Kazdin, 2005).
Taking it personally. This is perhaps the hardest point. When a learner says hurtful things, refuses your help or undermines your authority in front of colleagues, it is natural to feel angry, frustrated or defeated. But the child is not doing this to you. They are doing it because their brain is wired for conflict with authority, and they lack the self-regulation skills to respond differently. Separating the behaviour from the child is not just a therapeutic principle. It is a survival strategy for your own wellbeing.
The SEND Code of Practice (2015) sets out a graduated approach to meeting the needs of learners with special educational needs. This applies to ODD just as it applies to dyslexia, speech and language difficulties or any other area of need. The framework is known as the Assess, Plan, Do, Review (APDR) cycle, and it gives schools a structured way to move beyond reactive behaviour management towards planned, evidence-informed provision.
| DSM-5 Symptom Cluster | What You Might See in School | Frequency Threshold |
|---|---|---|
| Angry/Irritable Mood | Frequent temper outbursts over minor issues; easily annoyed by peers; persistent resentful or angry mood across the school day | Most days, for at least 6 months |
| Argumentative/Defiant Behaviour | Argues with teachers over routine instructions; actively refuses to follow classroom rules; deliberately provokes other learners; blames others for own mistakes or behaviour | At least weekly, for at least 6 months |
| Vindictiveness | Spiteful comments or actions aimed at peers or staff; holds grudges; retaliatory behaviour after perceived slights | At least twice in the past 6 months |
Assess. Gather baseline data. How often do oppositional behaviours occur? In which lessons? With which adults? Are there specific triggers (transitions, unstructured time, particular subjects)? Use an ABC chart (Antecedent, Behaviour, Consequence) to map patterns. Involve the learner where possible. Ask them what makes school hard. You may be surprised by the insight they offer. This assessment phase connects directly to your SEMH provision and should involve your SENCo from the outset.
Plan. Based on your assessment, create a targeted behaviour plan. This should specify: the key behaviours you are addressing (no more than two or three at a time), the strategies you will use (drawn from the evidence-based table above), the adults responsible, the review date and the success criteria. Be specific. "Improve behaviour" is not a target. "Reduce the number of lesson refusals from five per day to two per day within four weeks" is. Record this in your provision map.
Do. Implement the plan consistently. Every adult who works with the learner must know the plan and follow it. This is where one-page profiles are invaluable. They summarise the child's triggers, preferred strategies and de-escalation approaches on a single sheet that can be shared with cover teachers and support staff. Monitor as you go. Keep brief daily notes on incidents and successes.
Review. At the agreed review date (typically every six to eight weeks), assess progress against your success criteria. Has the frequency of oppositional behaviour decreased? Have new patterns emerged? Is the child engaging more in learning? If progress is sufficient, continue the current plan. If not, adjust. If you have been through two or three APDR cycles with limited improvement, this is the point at which to consider requesting an external assessment from an educational psychologist or referral to CAMHS.
The APDR cycle is not bureaucracy for its own sake. It is the mechanism that allows you to demonstrate what you have tried, what has worked and what has not. If a learner eventually needs an Education, Health and Care Plan (EHCP), your APDR records are the evidence base that supports the application.
ODD does not exist only in school. Parents and carers are dealing with the same behaviours at home, often without the training or support systems that schools have. Building a genuine partnership with the family is one of the most powerful things you can do for a learner with ODD. It is also one of the most difficult.
| Situation | Strategy | Why It Works for ODD |
|---|---|---|
| Lesson transitions | Give a 2-minute warning before any change of activity. Use a visual timer. State exactly what will happen next. | Reduces the surprise and loss of control that triggers defiance. Predictability lowers arousal. |
| Giving instructions | Offer limited choices: "Would you like to start with the diagram or the written questions?" Avoid open-ended demands. | Gives the learner a sense of autonomy within your boundaries. Reduces power struggles. |
| Refusal to work | Acknowledge the feeling ("I can see this is frustrating"), restate the expectation calmly, offer a reduced first step. Walk away briefly to allow processing time. | Validates emotion without endorsing the refusal. The walk-away prevents escalation and removes the audience. |
| Arguing with you | State the rule once. State the consequence once. Do not repeat or engage in debate. Use the phrase "I've told you what I need. I'll check back in two minutes." | Removes the argument loop. Learners with ODD are skilled at drawing adults into extended verbal battles. |
| Escalating anger | Lower your voice. Reduce your physical proximity. Offer a planned exit: "You can take five minutes in the reading corner." Have a pre-agreed calm-down routine. | Matching intensity fuels the cycle. A calm, low-energy response interrupts the escalation pattern. |
| After an incident | Wait until the learner is fully calm (20-30 minutes minimum). Use a restorative conversation: "What happened? What were you feeling? What could we do differently next time?" | Learners with ODD cannot process consequences or reflect while still in a heightened state. Timing is everything. |
| Daily relationship-building | Greet the learner by name at the door. Find one genuine positive comment per lesson. Refer to their interests. Invest in the 2:1 ratio (two positive interactions for every corrective one). | ODD learners often expect conflict from adults. A consistent positive relationship disrupts this expectation and builds trust over time. |
| Reinforcing positive behaviour | Catch them being good. Use specific praise: "You started that task within 30 seconds. Well done." Avoid generic praise ("Good boy"). Consider a private reward system rather than public charts. | Specific, immediate reinforcement builds the neural pathways for compliant behaviour. Private systems avoid the public humiliation that can trigger defiance. |
| Consistent boundaries | Apply the same rules and consequences every time, without exception. Share your approach with all adults who work with the child. Write it into a one-page profile. | Inconsistency is the enemy. If a learner with ODD discovers that defiance sometimes works, they will increase it. Consistency removes the incentive to test. |
Start by recognising that many parents of children with ODD have had negative experiences with schools. They may have been called in repeatedly for meetings that feel like blame sessions. They may have been told their child is "naughty" or that they need to "be firmer at home." By the time they reach your classroom, their defences may be as high as their child's. Lead with empathy. Start every conversation with something positive about their child. Ask about what works at home before offering advice.
Consistency between home and school is the gold standard for ODD management. If you are using a reward system in class, share it with the family and ask if they can mirror it at home. If you have identified specific triggers, compare notes. Some families find that the same strategies that work in the classroom, such as limited choices, advance warnings and consistent consequences, are effective at home too.
Refer learners to CAMHS if their behaviour greatly affects learning and wellbeing, despite school support. GPs often make referrals, but some areas allow schools to refer directly. Explain the referral process honestly to parents. UK waiting lists are long, so refer early. School support like counselling helps while waiting (Ford et al., 2007).
Incredible Years and Triple P are parent training programmes some schools find successful. These programmes, recommended by NICE, teach behaviour management techniques. Early Help services from your local authority might provide them (Webster-Stratton, 1990; Sanders, 1999).
ODD presents as defiant behaviour toward authority figures. Classroom signs and support tips are in the table. Teachers should be consistent and praise learners. Avoid power struggles, as Hinshaw and Anderson (2022) suggest.
Structural Learning ODD Strategies Guide says use strategies consistently at home and school. ODD is a recognised behavioural disorder needing consistent approaches. CAMHS or educational psychologists can give professional support for persistent problems.
| Symptom | How It Presents | Recommended Strategy |
|---|---|---|
| Angry or Irritable Mood | Frequent temper tantrums, easily annoyed, often angry and resentful | Remain calm, use positive reinforcement, avoid power struggles |
| Argumentative or Defiant Behaviour | Often argues with authority figures, actively defies or refuses to comply with rules, deliberately annoys others | Set clear and consistent rules, provide choices to reduce power struggles, use time-outs when necessary |
| Vindictiveness | Spiteful or vindictive behaviour, holds grudges | Address behaviours calmly, avoid retaliation, encourage empathy and understanding |
| Blaming Others | Often blames others for their own mistakes or misbehaviour | Help them understand consequences, teach responsibility, use problem-solving techniques |
| Easily Annoyed | Easily irritated by peers and adults, low tolerance for frustration | Teach coping skills, use relaxation techniques, create a low-stress environment |
| Frequent Anger Outbursts | Loses temper frequently, difficulty managing anger in the classroom | Teach anger management strategies, use calming techniques, provide a safe space for cooling down |
| Refusal to Follow Rules | Consistently disobeys rules and requests from adults | Implement consistent discipline, use a reward system for compliance, provide clear expectations |
| Frequent Blaming | Regularly blames others for their own behaviour or mistakes | Encourage taking responsibility, discuss the impact of actions on others, use role-playing to teach empathy |
| Frequent Resentment | Holds onto grudges, often resentful or spiteful towards peers and staff | Teach forgiveness and letting go, encourage positive social interactions, reinforce positive behaviour |
| Dealing with Authority | Defiance towards authority figures, frequent arguments with teachers and parents | Build a positive relationship, avoid confrontat ions, use problem-solving approaches |
| Understanding and Acceptance | ODD is a behavioural disorder, not a choice; learners need empathy and understanding | Educate yourself about ODD, validate feelings, maintain a supportive attitude |
| Adapted Communication | Emotional reactions from adults can escalate situations; language and tone matter | Use clear and concise language, avoid emotional reactions, remain calm and neutral, provide specific feedback |
| Consistent Discipline | Inconsistent consequences lead to confusion and increased defiance | Use consistent and fair discipline, establish a routine, provide immediate consequences |
| Positive Reinforcement | Learners with ODD respond better to recognition of positive behaviour than to punishment | Implement a reward system, praise specific positive behaviours, provide tangible incentives |
| Professional Support | ODD often co-occurs with ADHD, anxiety or conduct disorder and requires specialist input | Seek professional guidance, involve school support services, consider family therapy |
| Parent Training | Consistency between home and school is essential for managing ODD behaviours | Attend parenting classes, learn behaviour management strategies, seek support groups |
Professional learning supports teachers in managing oppositional behaviour, drawing on evidence-based programmes such as the Incredible Years (Webster-Stratton & Reid, 2010) and Triple P (Sanders, 1999). These resources help you teach learners more effectively.
ODD is not a label to fear. It is a condition to understand. With the right knowledge, consistent strategies and a commitment to seeing the child behind the behaviour, you can make a genuine difference to their school experience and long-term outcomes. The learners who push back the hardest are often the ones who need your patience the most.