Updated on
July 3, 2026
ADHD in the Classroom: 12 Strategies That Actually Work
12 evidence-based ADHD strategies for teachers: seating adjustments, task chunking, classroom scripts, common mistakes, and what the research says really works.


Updated on
July 3, 2026
12 evidence-based ADHD strategies for teachers: seating adjustments, task chunking, classroom scripts, common mistakes, and what the research says really works.
ADHD is the most common neurodevelopmental condition in UK classrooms, affecting roughly 5% of school-age children (NICE, 2018). For example, a Year 4 child with ADHD may struggle to hold multi-step instructions in working memory while inhibiting the urge to shout out an answer. Yet most teacher training covers it in a single session, if at all. The result is a gap between what teachers observe and what they understand about the cognitive mechanisms driving those observations.
This guide connects the brain science of ADHD directly to classroom practice. Each strategy section explains the underlying cognitive deficit first, then provides specific techniques grounded in that mechanism. You'll also find an interactive pathway finder tool to identify the right starting point for individual learners.
Barkley (1997) suggests ADHD is not an attention deficit. His Behavioural Inhibition Model sees it as an executive function disorder. Learners struggle to control their attention, not just pay attention.
Brown (2017) highlights a key "performance gap". This means learners with ADHD often understand the content, but still struggle to show it in class.
A Year 5 learner can ace photosynthesis verbally. Yet they may fail on a worksheet soon after. The knowledge is there, but retrieval is unreliable.
When teachers interpret this inconsistency as laziness or defiance, they respond with effort-based interventions: "Try harder," "If you just focussed," "You could do it yesterday, so you can do it today." These appeals target motivation. But ADHD is not a motivation problem. It's a self-regulation problem (Barkley, 2015). The brake system is unreliable, regardless of how much the driver wants to stop.
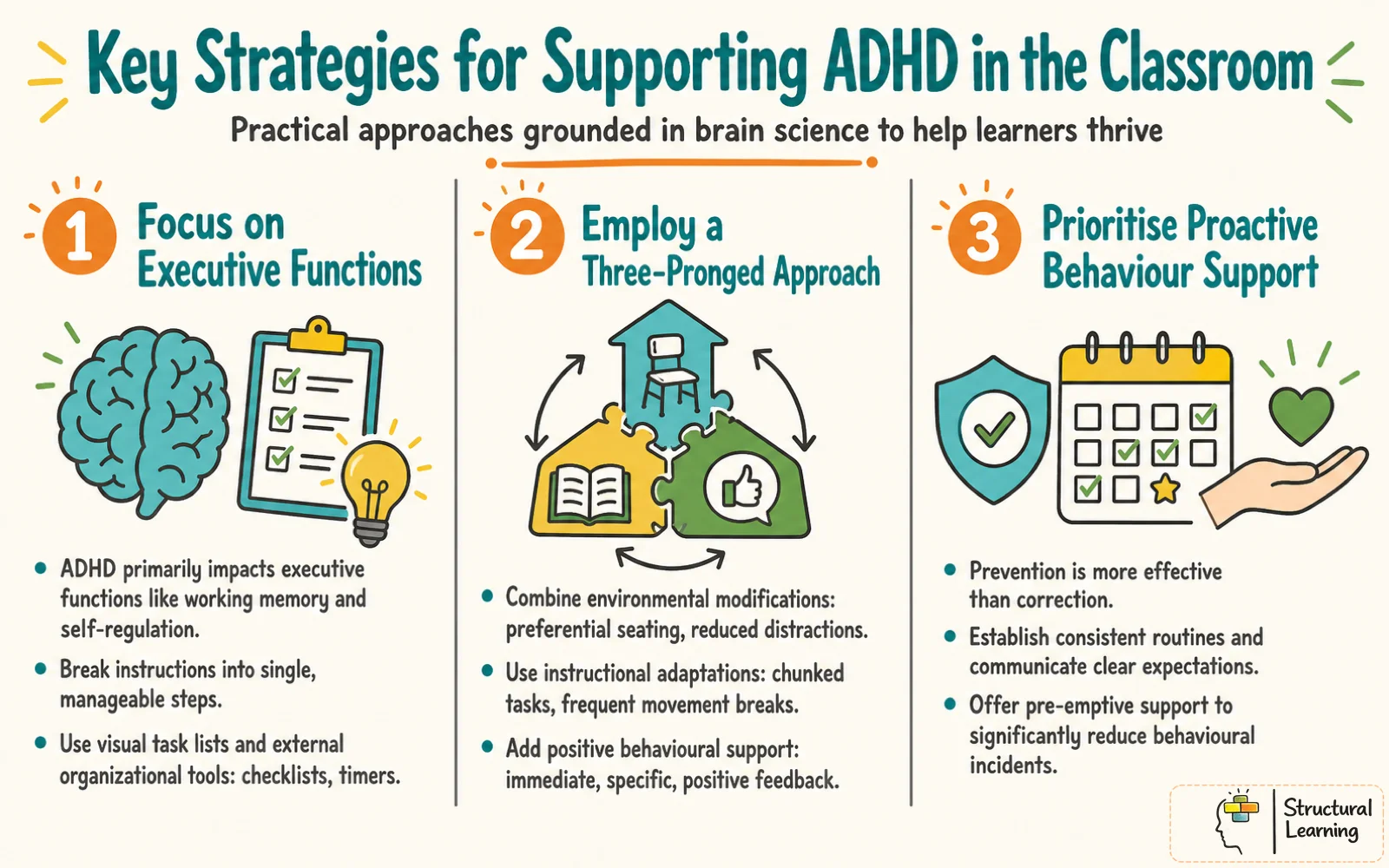
ADHD affects executive function, so strategies should address that, not willpower. This idea from cognitive science supports every recommendation here. Instead of asking for more effort, adapt the environment. Reduce executive demands so they fit the learner's current capabilities (Brown, 2017; Barkley, 2012).
UK Educator? These evidence-based ADHD strategies work in any classroom. For UK-specific SEND processes and how to record ADHD support formally, see our SENCO Role Guide and Provision Maps for SEN.
Diamond (2013) named three key executive functions: inhibitory control, working memory, and cognitive flexibility. ADHD can affect these functions in learners. Diamond (2013) also noted that poor inhibitory control often shows up in classrooms.
Think of inhibitory control as the brain's braking system. It's the mechanism that allows you to stop yourself from saying the first thing that comes to mind, to wait your turn, to resist reaching for your neighbour's rubber, to suppress an emotional reaction that isn't appropriate for the situation. In most learners, this system operates automatically and quickly. In learners with ADHD, the braking system is delayed and inconsistent (Nigg, 2017).
A Year 3 teacher asks the class a question. A learner with ADHD blurts out the answer before anyone else has raised a hand. This is not rudeness, and it is not a planned choice to break the rule.
The thought-to-speech pathway fires before the inhibitory system can stop it. The learner often looks surprised by their own outburst, which is diagnostically revealing. They did not choose to blurt, because their brake pedal responded too slowly.
Diamond (2013) distinguishes key forms of inhibitory control:
Different classroom behaviours can show different executive-function needs. Movement breaks may help with arousal or restlessness. However, they may not help a learner filter distractions or regulate frustration. This is why generic ADHD strategy lists often fail: the strategy must match the barrier you can see.

Martinussen et al. (2005) showed working memory problems are key in ADHD. Their meta-analysis included 26 studies. These memory deficits can really harm the learner. They are not just a side effect.
Baddeley's model (Baddeley, 2000) shows working memory has limits. The phonological loop holds words, and the visuospatial sketchpad holds images. The central executive links them but struggles in learners with ADHD. It finds it hard to manage information and process new input.
Picture this in practice. A teacher gives three instructions: "Open your textbook to page 42, read the passage silently, then answer questions 1 to 3 in your exercise book." A learner with working memory deficits may successfully hold "page 42" and "read silently" but lose "questions 1 to 3" before they've even found their textbook. By the time they've completed step one, the remaining instructions have evaporated.
Gathercole and Alloway (2008) linked working memory issues in ADHD to learning problems. Learners with ADHD struggle with tasks needing much working memory (Gathercole & Alloway, 2008). This happens even if learners understand the subject matter fully.
Sweller (1988) argued that problem solving can impose heavy cognitive load; in classrooms, multi-step mathematics and extended writing can similarly overload working memory when support is weak. Reduce the memory demands of the task instead of expecting learners to increase their capacity. Research by Kirschner, Sweller, and Clark (2006) supports this strategy.
Hattie's (2009) research reviewed over 800 meta-analyses. It shows which teaching strategies affect learner outcomes. His work identifies approaches that have strong effects on learner progress.
Use this interactive checklist to select classroom adjustments for individual learners with ADHD. Choose the strategies that match your learner's presentation, then generate a printable PDF to share with colleagues, parents, or keep in your SEND files.

Adapt instruction for ADHD by using strong teaching routines that help all learners. Rosenshine (2012) recommends presenting new material in small steps, with checks for understanding before moving on. For a learner with ADHD, this reduces working-memory pressure and makes it easier to restart after distraction.
Instead of teaching a full concept and then checking understanding, break the explanation into two-minute segments with a quick comprehension check after each. "Put your thumb up if you can tell me the first step." This approach reduces the working memory load at any single point and provides the teacher with immediate feedback about whether the learner is tracking.
Model your thinking when answering inference questions. Say: "Read the question, find the paragraph, think about the author's meaning." This shows planning steps ADHD learners struggle with (EEF, 2018). EEF rates metacognition and self-regulation approaches as high impact, at around eight months' additional progress on average, and its guidance recommends explicit teaching, modelling and scaffolding of metacognitive strategies.
The cognitive load research (Sweller, 1988) is clear: studying a worked example is cognitively less demanding than solving an equivalent problem. For ADHD learners, this reduction in demand is the difference between productive learning and frustrated shutdown. Present the worked example, discuss each step, then gradually fade the support across subsequent practice items.
The classroom environment imposes a constant cognitive load. This is why the CDC, Understood, HelpGuide.org and East and North Hertfordshire NHS Trust all start with similar practical moves: strategic seating, quieter work areas, visual schedules, task chunking and movement breaks. For learners with ADHD, these changes protect working memory resources that should be directed at learning.
DuPaul and Stoner (2014) suggest auditing classrooms for extra stimulation. Noisy corridors and scraping chairs create demands. These distractions add up for learners. Decide which displays help learning, and which are visual clutter.
Face-to-face group seating maximises social distractors. For focussed independent work, rows or paired desks reduce the number of faces, movements, and conversations competing for the learner's attention. This doesn't mean abandoning group work. It means intentionally varying the layout to match the cognitive demands of the task.
Learners can move between a reading corner, standing desk or quiet booth when the task demands change. NICE (2018) recommends environmental modification as part of first-line support. Use these spaces as planned regulation points, not as informal exclusion or a substitute for assessment.
Learners with ADHD often struggle with metacognition, which can worsen executive function (Reid et al., 2005). Metacognition means thinking about your own thinking, and it relies on working memory. When working memory is reduced, learners find it harder to monitor their work.
Rather than expecting ADHD learners to monitor their work in their heads, give them external prompts. A self-checking card on the desk ("Did I read the question? Did I answer all parts? Did I check my spelling?") moves that monitoring task from working memory into the environment. Hacker et al. (2009) found that explicit metacognitive instruction significantly improved academic performance in learners with attention difficulties.
Learners check work with partners after tasks (Topping (Topping, 2018), 2018). This "check and compare" takes two minutes. Partners offer support because learners' thinking skills are still developing (Vygotsky, 1978; Wood, Bruner & Ross, 1976).
Modelling your thinking shows metacognition in action ("Does my answer fit the question?"). For learners with ADHD, this clear example is key. Executive function deficits can impair self-monitoring (Brown, 2006; Barkley, 1997).
Teachers need to understand the difference between what a learner knows and what they show in their work. Learners with ADHD may understand concepts, but struggle with executive function under pressure (Barkley, 1997). Teachers could misread this inconsistency as laziness, not a regulatory issue (Brown, 2006; Goldstein & Ellison, 2002).
Cognitive load reduces when teachers move information outside the learner's mind. Visual schedules and timers give constant support (Sweller, 1988). Split instructions into steps; this prevents working memory overload (Chandler & Sweller, 1991).
Research shows that inhibitory control helps learners pause before they act (Diamond, 2010). Inhibitory control means the brain's brake system. This helps teachers see calling out as a neurological delay, not defiance (Casey et al., 1997). Teachers can then change the classroom set-up instead of punishing the learner (Blair & Raver, 2016).
Cognitive science sees ADHD as an executive function issue, not low motivation. The brain struggles to control behaviour and attention reliably. Therefore, interventions relying on effort often fail (Brown, 2005; Barkley, 2012). They target the wrong brain functions (Diamond, 2016).
Teachers often use strategies that don't suit all learners. Movement breaks won't aid a learner with inattention. Motivational talks, without support, also fail learners (Vygotsky, 1978; Piaget, 1936).
Adults need to support learners who have emotional dysregulation and ADHD. Teachers can model calm reactions and co-regulate first, before they expect self-regulation. Clear routines and predictable settings also help reduce transitions (Barkley, 1997).
Medicated learners are in your classes. You are not prescribers, yet understanding medication is key. Knowledge of medication helps create fair classroom expectations. Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
Stimulant medicines increase dopamine and noradrenaline (Cortese et al., 2018). This helps the learner focus, remember facts, and control themselves. Medication does not change personality, knowledge, or motivation. It helps the brain regulate its functions more effectively.
Medication can make attention and inhibition more reliable, but it does not teach planning, self-checking or task initiation. If ADHD has disrupted years of practice, the learner still needs explicit metacognitive teaching and classroom scaffolds (NICE CG87, 2018). Pair any medication plan with visible routines, feedback and skill practice.
Teachers see medication effects throughout the school day. A learner's focus can improve in the morning, but decrease after lunch. This gives important information to the prescribing doctor (Vitiello et al., 2001).
Note facts: "Completed three tasks before break. After lunch: incomplete work, off-task." Share observations via the SENCO. This helps medication management (Brown et al., 2005) without you making diagnoses (Evans et al., 2014).
Classroom strategies can support learning, but they do not replace clinical assessment or medication review. If concerns are severe or do not improve, record facts you can observe. Share them through the SENCO and follow local referral routes. Diagnosis and treatment decisions should stay with qualified clinicians and families.
Write to a learner you're concerned about this week. Note what you observe, not what you interpret. Share it with your SENCO. That single action often starts the process that leads to the right support.
The executive-function account of ADHD is useful, but it can become too narrow. Sonuga-Barke (2002) argued that delay aversion and reward sensitivity can operate alongside inhibition problems, so a learner avoiding a long writing task may be protecting themselves from delay, boredom or shame, not simply forgetting the next step.
Cognitive load theory also needs careful use. Sweller (1988) and Kirschner, Sweller and Clark (2006) support explicit guidance when task load is high, but Hmelo-Silver, Duncan and Chinn (2007) warned that well-scaffolded inquiry is not the same as unguided discovery. Teachers should reduce unnecessary load without turning every lesson into tightly controlled talk.
Some common accommodations have weak transfer to academic outcomes. Lovett (2010) argued that extended-time decisions should be tied to a measured functional barrier, not a label alone. Recent reviews also show uneven effects: school-based ADHD interventions improve inattention and academic performance more reliably than hyperactivity, and social-skills programmes can show negligible effects (Yegencik et al., 2025; Bussanich et al., 2025).
The evidence base remains culturally and methodologically limited. Karpicke (2008) used controlled retrieval tasks, Vygotsky (1978) is often applied across cultures without enough attention to language and authority norms, and Gillborn and Youdell (2000) showed how race and class can shape teacher judgement. Despite these limits, the cognitive-science frame still has enduring value because it shifts classroom support from blame to designed scaffolding.
Karpicke, J. (2008). The critical importance of retrieval for learning.
Kirschner, P. (2006). Why minimal guidance during instruction does not work.
Sweller, J. (1988). Cognitive load during problem solving.
Vygotsky, L. (1978). Mind in society: The development of higher psychological processes.
These sources separate clinical guidance from classroom support and link to traceable DOI, PubMed, ERIC, publisher or official guidance pages.