







Updated on
July 2, 2026
Trauma-Informed Teaching: A Practical Guide
Trauma-informed teaching in schools: what ACEs are, how to spot trauma responses in the classroom, and practical strategies for whole-school practice.


Updated on
July 2, 2026
Trauma-informed teaching in schools: what ACEs are, how to spot trauma responses in the classroom, and practical strategies for whole-school practice.
Trauma-Informed Teaching: A Practical Guide describes how teachers can reduce avoidable stress responses. At the same time, it keeps learning purposeful, structured, and fair. It treats trauma as a possible influence on attention, trust, attendance, memory, and behaviour, not as a label for a learner. Evidence from adverse childhood experiences research is important, but ACE data were designed for population-level public health analysis, not classroom diagnosis (Felitti et al., 1998; Anda, Porter and Brown, 2020).
Trauma-informed teaching means that school staff understand how adversity may affect learning, behaviour, attendance, and relationships. They then use predictable routines, relational safety, and proportionate support, which means help that matches the need. This should not mean diagnosing learners or lowering expectations.
In practice, this means pairing calm relationships with clear routines: for example, a Year 6 learner who shuts down when corrected may need a predictable private prompt, a short reset, and a clear route back into the task. Trauma-informed teaching is strongest when it protects dignity, maintains high expectations, and helps staff respond consistently rather than excuse unsafe behaviour.
Create safer classrooms, offering more support. Perry (2009) and Wolpow (2016) found trauma affects learning. Consider learners' backgrounds, not just punishing behaviour. Trauma-informed teachers ask, "What happened to this learner?"
The ACE Study (Felitti et al., 1998) surveyed 17,000 adults. This showed childhood adversity directly linked to later problems. Neuroscience (Perry, 2006) showed chronic stress changes the developing brain. Schools used this science to rethink how they manage learner behaviour.
Bomber (2007) advised UK teachers on learner behaviour. She linked it to early attachment issues. Bomber stated school staff support learners' emotions. They act as secondary attachment figures.
This approach considers how trauma affects learners. Teachers understand emotional and brain barriers (Perry, 2009).
We change teaching to lessen these barriers (Cole et al., 2005). Learners need safe, structured classes (Bloom, 2010). Teachers keep expectations high and manage behaviour fairly.
ACEs are traumatic events before age 18. Felitti et al. (1998) found abuse, neglect, and household issues. Abuse covers physical, emotional, and sexual forms.
Felitti et al. (1998) link household issues to violence or substance misuse. Anda et al. (2006) include parental illness, jail, or divorce.
Felitti et al. (1998) found that ACEs are common: roughly two-thirds of participants reported at least one ACE, and one in eight reported four or more. The study established an ACE score, a count of distinct categories of adversity, and showed that the higher the score, the worse the outcomes across virtually every domain measured.
Van der Kolk (2014) found early trauma changes the brain. Trauma affects the amygdala, prefrontal cortex, and hippocampus. Learners with trauma have brains wired for survival, hindering learning.
In practical terms, this means a traumatised child may:
Perry's neurosequential model (Perry, 2006) adds that the brain develops from the bottom up: the brainstem (survival) develops before the limbic system (emotion), which develops before the cortex (reasoning). A child in a state of threat is operating from the lower brain. No amount of reasoning, consequence, or reward will reach the cortex until the lower brain is regulated first.
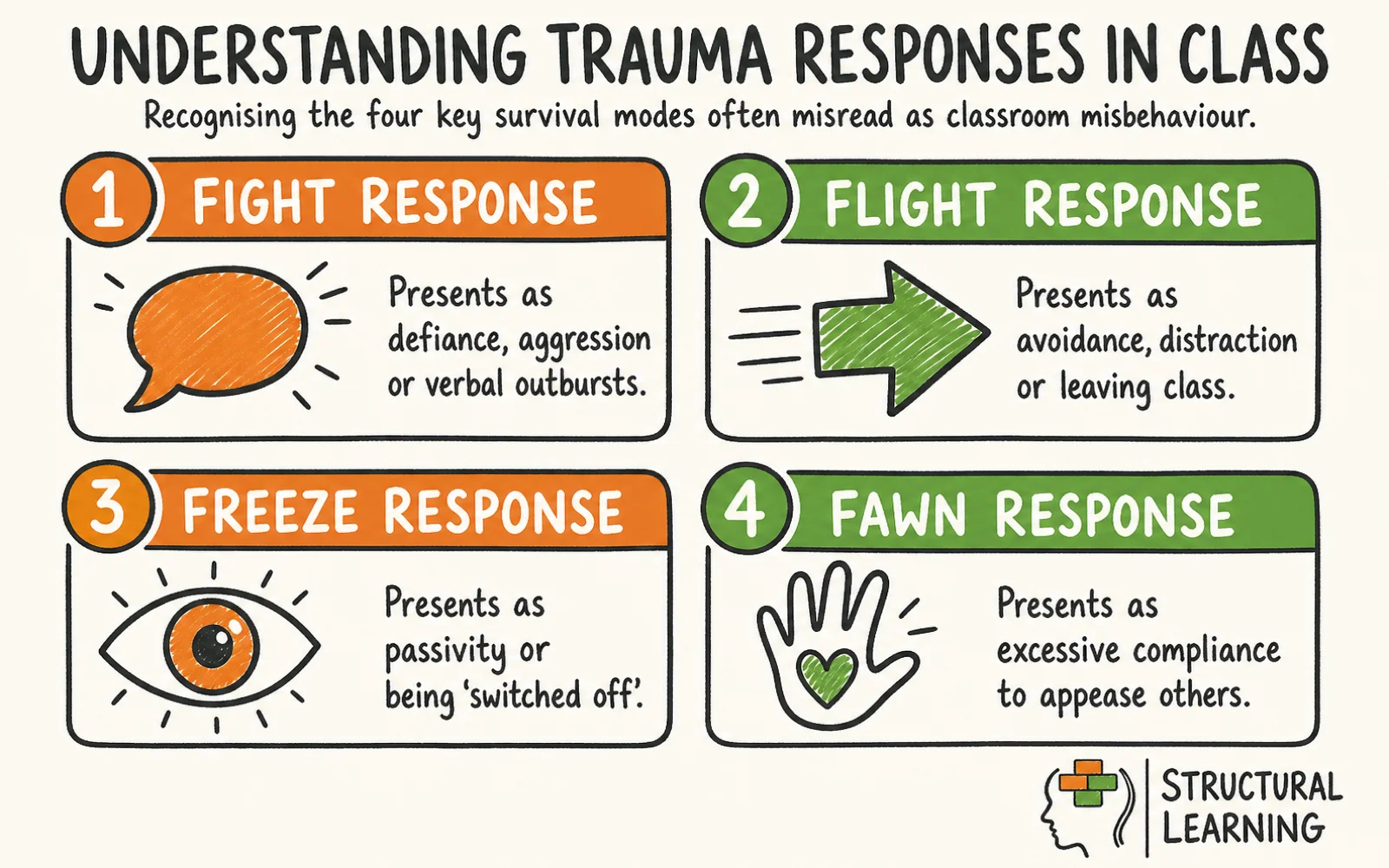
Trauma responses (fight, flight, freeze, fawn) confuse teachers. Van der Kolk (2014) says these are automatic survival strategies. Ogden (2012) notes these are neurological reactions, not misbehaviour. Understand this to better support each learner (Porges, 2011; Levine, 1997).
Fight responses present as aggression, defiance, verbal outbursts, or throwing objects. The child is not choosing to be difficult. Their nervous system has detected a threat and is mobilising for attack. Common triggers include perceived humiliation, unexpected changes, raised voices, or being singled out in front of peers.
Flight responses present as avoidance, leaving the room without permission, or persistent refusal. The child is attempting to escape the perceived threat. In quieter forms, flight looks like distraction, doodling, or disengagement from tasks they find overwhelming.
Freeze responses present as apparent passivity, blank expression, inability to respond to questions, or seeming 'switched off'. The child is neither fighting nor fleeing; their nervous system has shut down in the face of an overwhelming threat. Freeze is frequently misread as laziness, defiance, or low ability.
Fawn responses mean learners excessively please people. They show compulsive compliance or cannot say what they want. The learner thinks safety means appeasing others.
Fawn responses are hard to spot; learners seem cooperative. However, they could be hiding significant distress (Ford, 2003).
Perry (2006) asks: "Can this learner's brain learn right now?". If not, co-regulation comes before teaching. Bomb (Bomber, 2007) suggests 'settling activities'. These brief tasks create safety before learning restarts.
SAMHSA (2014) outlined six core principles for trauma-informed care. These principles, used in health, now appear in schools. Consider how they help learners. Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
Perry et al. (1995) found consistent routines and clear rules build learner safety. Calm, predictable teacher actions boost these feelings. Siegel (2010) showed this is vital when a learner faces challenges.
Transparency is key: explain decisions clearly to learners. Unpredictability threatens learners with developmental trauma. Advance notice of changes and keeping promises builds trust (Porges, 2011; Cook et al., 2005). Honesty when things go wrong also matters (Hughes, 2008).
Peer support uses learner relationships as a resource. Structured group work, restorative chats, and teaching social skills help learners. These build social skills damaged by trauma (Bath, 2008; Howard, 2018).
Researchers such as Perry (2006) suggest minimising power differences between teachers and learners where suitable. Give learners control in their learning. This acknowledges some learners experience trauma from a lack of power, according to Cairns (2002). Meaningful choices can help learners with this, as noted by Saleeby (1996).
5. Empowerment, voice, and choice. Strengths are identified and built on. Learners are helped to develop skills and recognise their own competence. Bomber (2007) argues that many traumatised children have an impaired sense of self-efficacy; small, structured opportunities to experience success can begin to repair this.
Culture, history, and gender affect learning. Trauma affects marginalised learners (van der Kolk, 2014; Perry & Szalavitz, 2006), so practice should recognise racism and poverty. Think about each learner's background.
These six principles are not a checklist to complete once. They are ongoing commitments that need to be embedded in policy, staff training, behaviour management procedures, and day-to-day classroom practice.
Bomber (2007), Perry (2006), and SAMHSA (2014) offer practical, evidence-based approaches. These strategies help you support learners in your classroom. Use them! Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
Traumatised children need the world to be predictable. Begin every lesson with the same brief settling activity: reading a short passage, completing a low-stakes retrieval task, or spending two minutes on a journal prompt. End lessons with a clear signal and a consistent farewell.
Display a visual timetable so transitions are never a surprise. Even small deviations from routine can dysregulate a vulnerable child, so when changes are unavoidable, give as much advance warning as possible.
Perry's neurosequential model (2006) tells us that a dysregulated child cannot access higher cognitive functions. Before attempting to teach a child who is visibly distressed, help them regulate.
This might mean a brief walk to the water fountain, a quiet corner with a sensory resource, or simply sitting alongside them in silence for a minute before asking a low-demand question. Regulation is not a reward for poor behaviour. It is a prerequisite for learning.
Rogers (1951) and unconditional positive regard are useful. Traumatised learners think adults see them as bad.
Show warmth and interest to challenge this idea. This isn't accepting bad behaviour. Separate the learner from what they did.
Co-regulation, the process by which a regulated adult helps a dysregulated child return to a calm state, is not only a clinical skill (Schore, 2001). It is something every teacher can practise.
Lower your own voice when a child escalates. Slow your speech. Use open, non-threatening body language. Avoid direct eye contact if it reads as confrontational.
When you demonstrate calm, you are providing a neurological model that the child's developing nervous system can begin to mirror.
Giving traumatised children meaningful choices reduces the neurological impact of powerlessness. "You can do this task sitting at your desk or on the floor with a clipboard. Which would you prefer?" is a small act. For a child whose life has been characterised by a lack of control, it is significant. Choices should always be real and limited: two or three options, not an open invitation.
Bomber (2007) links difficult behaviour to learner attachment needs, which means needs linked to trust and close relationships. Learners may break rules to get attention, and this can show relationship problems. Regular check-ins and reliable adults offer support. Positive attention lowers pressure and can reduce bad behaviour.
Trauma-informed practice needs school-wide changes, not just single methods. Systemic change helps learners more than classroom work alone (Cole et al., 2005; Thomas et al., 2019). Whole-school approaches to trauma-informed practice are widely recommended as more effective than classroom work alone, although the underlying evidence base is still emerging (Cole et al., 2005).
Staff need a shared understanding of ACEs and trauma (Bloom, 2016). All must learn to respond with curiosity, not punishment. Ongoing professional development and supervision are vital (Cole et al., 2005). Create a culture where staff discuss difficult situations openly (Bath, 2008).
Review behaviour policies, and check for practices that can make trauma worse for learners. Avoid public shaming and routine exclusion (Bloom, 2016), and use fewer rigid, zero-tolerance approaches (Perry & Szalavitz, 2017). Keep consequences fair, in proportion, and built around relationships (van der Kolk, 2014). Focus on repair, not just punishment (Bath, 2008).
Designated safe spaces within the school building provide regulated children with somewhere to go when overwhelmed. These spaces should be calm, predictable, and supervised by a consistent adult. They are not withdrawal rooms for bad behaviour. They are regulated environments that help children return to a state where learning is possible.
Leaders should identify vulnerable learners as part of standard pastoral practice, tracking patterns and providing proactive support rather than crisis response only. Referral pathways to CAMHS and local social care need to be clear to all staff, in line with the trauma-informed approach set out in the SAMHSA framework (SAMHSA, 2014).
Learners with trauma need emotional support. Teachers hear disclosures and see distress (Ford et al., 2012). They manage challenging behaviour too. This can cause vicarious trauma without support (Bride, 2007).
Figley (1995) defined vicarious trauma as repeated exposure to others' trauma. It differs from burnout, although they can happen together. Learners' experiences may affect teachers deeply. Symptoms include intrusive thoughts and sleep problems like direct trauma.
Schools have a duty of care to their staff as well as their learners. The following structures reduce the risk of vicarious trauma and support staff who are already affected.
Supervision gives staff time to discuss tricky cases with a colleague or manager. These sessions are regular and structured, not performance management (Proctor, 1986). Supervision offers a safe place for honest reflection (Morrison, 2005; Hawkins & Shohet, 2012). This helps the learner.
Clear role boundaries. Staff should understand what their role requires them to do and what it does not.
The teacher's role is to teach and to provide a safe, regulated classroom environment. It is not to act as a therapist. Clarity about this boundary protects staff from taking on more than they can sustain.
Researchers Stamm (2010) and Figley (1995) show vicarious trauma hurts staff. Training should include compassion fatigue information. Knowing the signs helps learners seek early support.
Schools must tell staff about employee assistance programmes. They should also provide counselling referrals and occupational health support. This ensures all staff have access to vital resources.
Leadership modelling. Senior leaders set the tone. If leaders speak openly about the emotional demands of the work, take rest seriously, and model self-care, they signal that wellbeing is valued.
If they do not, staff will not seek help even when they need it. For related guidance, see our article on Social-Emotional Learning and Wellbeing in Schools.
The teacher wellbeing and workload crisis in the UK (DfE, 2019) is not unrelated to the demands of working with increasingly complex learner needs. Addressing vicarious trauma is not a luxury. It is a workforce sustainability issue.
Schools need external support for childhood trauma (Cole et al., 2005). Trauma-informed practice means working with specialist agencies. These agencies provide important assistance that schools cannot (Perry, 2009). Build strong relationships with them.
Child and Adolescent Mental Health Services (CAMHS) are the most commonly referenced referral pathway, but waiting lists are long and thresholds are high in most areas. Teachers need to understand what CAMHS can and cannot offer so that referrals are appropriate and expectations are managed.
Educational psychologists assess learners, give advice, and plan support. They help schools tell the difference between trauma responses and conditions like autism (APA, 2013). ADHD and learning difficulties often occur together, so diagnosis can be more complex (Gillberg et al., 2004).
Schools must participate in child protection plans and team meetings if social care is involved. Sharing information well with social workers is vital for safeguarding. This forms a coordinated, trauma-informed approach (Steer et al., 2009).
Researchers note Place2Be and Young Minds offer school services. These charities ease teacher burden when funding exists. School-based therapists ensure learners receive expert support (Ford et al., 2017).
Research shows annual reviews can address trauma for learners with EHCPs. These meetings help ensure the plan reflects learner needs and coordinates support (Bowlby, 1969; Main, 1995; Prior & Glaser, 2006).
Even well-intentioned schools can make the same mistakes when they put trauma-informed practice into place. Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
Trauma-informed practice changes school culture for all learners. Trauma-specific help requires trained clinicians for specific learners. Teachers, like those discussed by Cole et al. (2005), aren't therapists. Blurring these roles risks burnout and weakens boundaries.
Embedding trauma-informed practice takes time. Schools might book a single training day, but that is not enough. Ongoing work is needed, incorporating supervision and policy reviews. Include this in new staff induction and reflective practice discussions (Bloom, 2016).
Some teachers over-correct and remove all structure to be kind. Traumatised learners need both warmth and consistent boundaries. Boundaries signal safety when applied with warmth. A lack of clear expectations destabilises learners.
Failing to address staff wellbeing. A school cannot be trauma-informed for learners if it is not also attentive to the wellbeing of its staff. Vicarious trauma that goes unaddressed damages staff and, ultimately, the quality of care they are able to provide.
This can harm learners (Perry & Hambrick, 2008). Trauma affects everyone, so all staff should understand it (Bloom, 2010). Leaving responsibility only with the SENCO limits wider impact (Cairns, 2000). Whole-school training helps create supportive environments (Cole et al., 2005).
Trauma-informed teaching starts with a question: not "What is wrong with this child?" but "What has happened to them?" That shift in framing changes everything that follows: how you read behaviour, how you design routines, how you respond to distress, and how you support your colleagues.
ACEs affect brain development (Hughes et al., 2015). Trauma-informed schools find better attendance and learner wellbeing. Schools need commitment, training and updated behaviour policies for this approach.
Your next step: identify two trauma-informed principles from the SAMHSA framework that your school already does well, and one where practice is inconsistent. Bring that reflection to your next team meeting as the starting point for a structured conversation.
Trauma-informed teaching has clear value, but it is not a complete theory of learning or behaviour. One limitation is the weak use of ACE scores in schools. Felitti et al. (1998) showed important population-level links between adversity and later health, but Anda, Porter and Brown (2020) warn that ACE counts should not be used to diagnose, profile, or predict outcomes for individual children.
Open a free account and help organise learners' thinking with evidence-based graphic organisers. Reduce cognitive load and guide schema building dynamically.
A second criticism is that trauma-informed practice can slip into deficit thinking. This means seeing learners mainly through what they lack. Miller and Flint-Stipp (2024) argue that the language of trauma may lead teachers to see learners as damaged or fragile. Ecclestone (2012) raises a related concern: therapeutic approaches can lower academic expectations when adults confuse psychological safety with reduced challenge.
There are also cultural and methodological limits, which means limits in who was studied and how the research was done. Much early trauma research used narrow samples. It gave less attention to racism, poverty, community violence, disability, and school exclusion. The Philadelphia ACE Study widened the frame by including community-level adversity, while Ginwright (2018) argues for healing-centred engagement that recognises identity, culture, agency, and collective harm.
Finally, the evidence for school programmes is mixed. This is because interventions vary widely, outcomes are measured in different ways, and staff wellbeing is often under-specified. Trauma-informed teaching is still useful when it is precise: it should protect dignity, maintain boundaries, support staff, and keep learners connected to ambitious learning.
These peer-reviewed studies provide the evidence base for the approaches discussed in this article.
Integrating Trauma-Informed Teaching and Learning Principles Into Nursing Education. View study ↗ 11 citations
C. Clark (2023)
Clark (2023) shows how trauma impacts learners and how trauma-informed methods can be embedded in classroom practice. UK teachers can use these methods to address the educational impact of inequality and health-related adversity, adapting lessons to support learners affected by trauma and building a more inclusive classroom culture.
APA (2013).
Bath (2008).
Bloom (2010).
Bloom (2016).
Bomber (2007).
Bride (2007).
Cairns (2000).
Cole et al. (2005).
DfE (2019).
Felitti et al. (1998).
Ford (2003).
Ford et al. (2012).
Ford et al. (2017).
Gillberg et al. (2004).
Hughes (2008).
Hughes et al. (2015).
Perry (2006).
Perry (2009).
Proctor (1986).
SAMHSA (2014).
Schore (2001).
Steer et al. (2009).



