Updated on
July 3, 2026
ADHD vs Autism vs PDA
Compare ADHD, autism, PDA and related conditions across six classroom domains. Learn to distinguish them and adjust your teaching with confidence.


Updated on
July 3, 2026
Compare ADHD, autism, PDA and related conditions across six classroom domains. Learn to distinguish them and adjust your teaching with confidence.
ADHD vs Autism vs PDA describes a classroom distinction that is easy to miss: attention regulation, autistic processing differences and anxiety-driven demand avoidance can look similar during the same lesson. A Year 4 learner stares out of the window during carpet time, fidgets, interrupts and avoids writing.
The teacher suspects ADHD. The SENCO also notices distress at unstructured break times and changes to routine, which points towards autism. At home, his parents describe extreme demand avoidance and distraction around everyday tasks, so PDA enters the picture.
ADHD vs Autism vs PDA compares three profiles that can look similar in class. ADHD mainly affects attention, inhibition and executive function. Autism affects social communication, sensory processing and the need for predictability.
PDA describes extreme demand avoidance linked to a felt loss of autonomy. It is usually discussed as a profile within autism, rather than as a separate formal diagnosis (Green et al., 2018; Kildahl et al., 2021).
This scenario plays out in UK classrooms every week. ADHD, autism and PDA are not neat boxes: the DSM-5 allowed dual ADHD-autism diagnoses, and PDA is still debated rather than recognised as a separate DSM-5-TR or ICD-11 category (American Psychiatric Association, 2013; Green et al., 2018; Kildahl et al., 2021).
Teachers observe behaviours, but the same behaviour can have different causes. A learner who "can't sit still" may have ADHD, autism, or both. A learner who refuses tasks may be protecting themselves from overload, anxiety, loss of autonomy, or an unidentified learning difficulty.
Neurodevelopmental profiles overlap because attention, sensory processing, emotional regulation and executive function are linked. Differences in prefrontal development can affect inhibition, working memory and impulse control. Sensory load can also push a learner into shutdown or distress (Kern et al., 2015). In class, the same refusal to start writing may reflect ADHD task initiation, autistic overload, a PDA profile, or a specific learning difficulty.
The DSM-5 removed the diagnostic exclusion that previously prevented dual ADHD-autism diagnoses (American Psychiatric Association, 2013). For more on this topic, see Conners rating scale teachers guide. This change acknowledged what teachers had long observed: ADHD and autism often co-occur rather than appearing as tidy, separate profiles. A meta-analysis by Rommelse et al. (2010) found shared genetic factors between ADHD and ASD, with siblings of autistic children showing higher ADHD traits than the population average.
For SENCOs, this clustering creates a practical problem: referral pathways are usually condition-specific, but classroom need is not. A CAMHS referral for ADHD follows one route, an autism assessment follows another, and demand avoidance often starts a third conversation; waiting for the perfect label leaves teachers managing distress without a plan. A transdiagnostic approach means tracking attention, sensory load, flexibility, autonomy and emotional recovery across labels, then putting low-arousal, high-flexibility support in place while referral evidence is gathered (Astle et al., 2022). The Symptom Overlap Matrix below helps you map what you observe before deciding where to refer.
When SENCOs understand the main features of each condition, they can tell similar classroom needs apart more clearly. Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
This complexity means teachers should look for patterns across categories, not search for a single neat cause. A learner may show attention differences, sensory distress and demand avoidance in the same week. Recording the trigger, setting, recovery time and successful adjustment gives a stronger picture of need than a label-only checklist.
Observable classroom behaviour can hide different causes. The six domains below separate what the teacher sees from what may be driving it, so a learner is not misread as careless, defiant or lazy when the barrier is attention, sensory load, anxiety or literacy access (Hinshaw, 2002; Barkley, 2006).
Social difficulties appear across multiple conditions, but the underlying mechanism differs. An autistic child may struggle to read facial expressions because of differences in social cognition (Baron-Cohen, 1997). A child with ADHD may miss social cues because they were not attending when the cue occurred. A child with a PDA profile may appear socially skilled in one-to-one interactions but struggle in group settings where demands increase.
What the teacher sees: A learner who talks over others during group work, stands too close to peers, or gives responses that seem unrelated to the conversation topic. All three conditions produce this behaviour, but the cause is different each time.
Observe if the learner's social struggles are constant (ASD) or shift with interest and arousal (ADHD). If the learner skillfully avoids work but finds real friendships hard, think PDA.
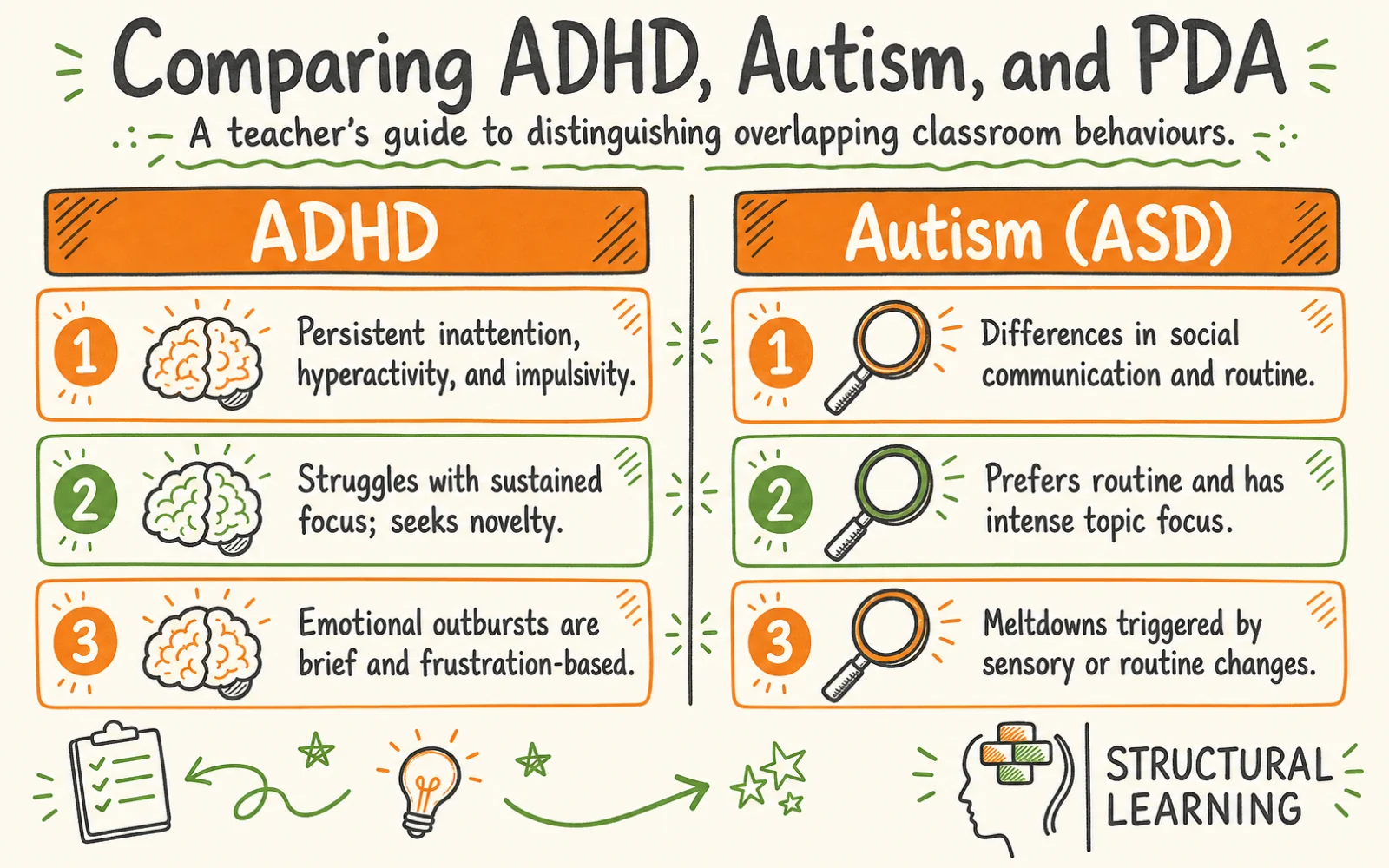
Inattention is common across conditions, says Barkley (1990). Autistic learners may seem inattentive in class but focus intensely on interests. Learners with SpLD may "zone out" when reading, explains Nicolson (2009). Decoding uses so much effort they cannot comprehend, notes Fawcett (1996).
What the teacher sees: A learner who stares out the window during teacher exposition but produces detailed artwork during free choice time.
Map the inattention pattern. Check for SpLD first if reading/writing tasks are hardest. ADHD is likelier if novelty improves attention across contexts. Autism fits better if the learner's attention is intensely narrow (Barkley, 2015).
Meltdowns, shutdowns, and emotional outbursts occur across ASD, ADHD, PDA, and ODD. The trigger and recovery pattern differ.
Autistic meltdowns often start with sensory overload or change (Mazefsky et al., 2013). Verbal calming may not work during this intense crisis.
ADHD learners' outbursts are often quick, from frustration, and soon pass. PDA distress rises when faced with demands, seeming like panic. ODD defiance targets adults and lasts longer.
What the teacher sees: A child who throws a chair during a maths lesson.
How to distinguish: Ask three questions: (1) Was there a sensory or routine trigger? (ASD) (2) Was the child asked to do something? (PDA) (3) Is this behaviour targeted at a specific adult and sustained? (ODD) (4) Did it resolve within minutes once the frustration passed? (ADHD)
Sensory processing differences are part of the autism diagnostic criteria (DSM-5). However, sensory distress also appears in ADHD, DCD/dyspraxia and PDA profiles (Ghanizadeh, 2011). A learner who covers their ears during alarms may be responding to auditory pain, loss of predictability, crowding, or a demand linked to the noise. Record the sensory trigger before treating the behaviour as non-compliance.
What the teacher sees: A learner who refuses to wear the school jumper, complains about classroom lighting, or becomes distressed in the dinner hall.
Researchers explain sensory difficulties in different ways. If the difficulty stays the same across places and is clearly linked to sound, touch, light or other senses, it may indicate ASD (Mazefsky et al., 2013). If the sensory issue changes with the learner's emotions, it could be ADHD (Ghanizadeh, 2011). If complaints increase when adults make demands, such as "wear your jumper", this may suggest demand avoidance.
Brown et al. (2017) found that executive function includes planning and organisation. Learners also need task initiation, working memory, and cognitive flexibility. Diamond (2013) notes that similar symptoms can appear in different situations. Goldstein et al. (2018) highlight significant overlap.
Barkley (2012) says ADHD affects inhibition, which means stopping an impulse, and working memory. Hill (2004) found that autistic learners can find cognitive flexibility, or shifting thinking, hard. PDA learners use executive functions when they lead the learning. For SpLD learners, executive function problems often come from managing learning needs.
These behaviours can point to different barriers. Some learners struggle to plan, organise materials or hold instructions in working memory; others can plan well when they choose the task but freeze when an adult imposes it (Meltzer, 2007; Levine, 2002; Diamond, 2013). Note whether support works better as a checklist, a model, a sensory adjustment or a choice-based invitation.
Consider PDA if a learner plans their own tasks well, but struggles with your activities. Check for SpLD if literacy/numeracy shows the biggest executive function problems. ADHD or ASD are possible if difficulties are widespread (Gillberg, 1992; Baron-Cohen, 1988).
Neurodevelopmental profiles can affect learning unevenly. A bright autistic learner may meet academic targets but still struggle with the classroom environment. A learner with dyslexia may show behaviour difficulties because reading or writing in front of others has become a public risk (Ford et al., 2003).
These discrepancies have been observed by researchers (e.g., Ganschow et al., 1992; Shaywitz, 1998). Teachers may see a learner whose writing is much weaker than their speaking. Alternatively, a learner may do well on tests yet avoid doing work in class.
Compare test scores with classroom work to spot differences. A large gap between verbal skills and writing may indicate SpLD. Learners who refuse tasks despite ability may have PDA (Newson et al., 2003). If performance differs day to day, consider ADHD (Antshel, 2018).
The interactive tool below allows you to select two or three conditions and compare their overlapping symptoms across all six domains. Select the conditions you are considering for a specific learner, and the matrix will highlight which symptoms are shared and which are unique to each condition.
Learners with a PDA profile often use charm, distraction, delay or excuses to avoid tasks (Newson et al., 2003; O'Nions et al., 2014). The key issue is not ordinary refusal, but a threat response when a demand feels like loss of autonomy. PDA is not a separate DSM-5-TR or ICD-11 diagnosis; it is usually discussed as a demand-avoidant profile within autism, although this classification remains disputed (Green et al., 2018; Kildahl et al., 2021). Some neurodiversity-affirming writers prefer terms such as Pervasive Drive for Autonomy or Rational Demand Avoidance because these name the need for control without labelling the learner as wilfully difficult (Milton and Woods, 2018).
Letter reversals alone do not diagnose a learning difficulty. However, ongoing barriers with reading, spelling or writing need careful assessment (Elliott & Grigorenko, 2014; Fawcett & Nicolson, 2007; Shaywitz & Shaywitz, 2005). Check whether the learner also has working memory, phonological processing or fluency difficulties (Alloway, 2009; Gathercole & Alloway, 2008). A literacy barrier can look like task refusal when the work feels exposing.
| Condition | Core Feature | What You See in the Classroom |
|---|---|---|
| Autism (ASD) | Differences in social communication and restricted/repetitive patterns | Misses social cues, prefers routine, intense topic focus, sensory sensitivity, literal interpretation of language |
| ADHD | Persistent inattention, hyperactivity, and impulsivity | Fidgets, blurts out answers, loses equipment, struggles with sustained focus, seeks novelty |
| PDA Profile | Extreme avoidance of everyday demands driven by anxiety | |
| ODD | Pattern of angry/irritable mood, argumentative behaviour, vindictiveness | Deliberately annoys others, refuses adult requests, blames others, loses temper frequently |
| SpLD | Specific difficulties with reading, writing, maths, or motor coordination |
Symptom Overlap Matrix
Compare two or three conditions across six classroom areas. This will help you identify shared symptoms. Download the PDF to support your APDR cycle.
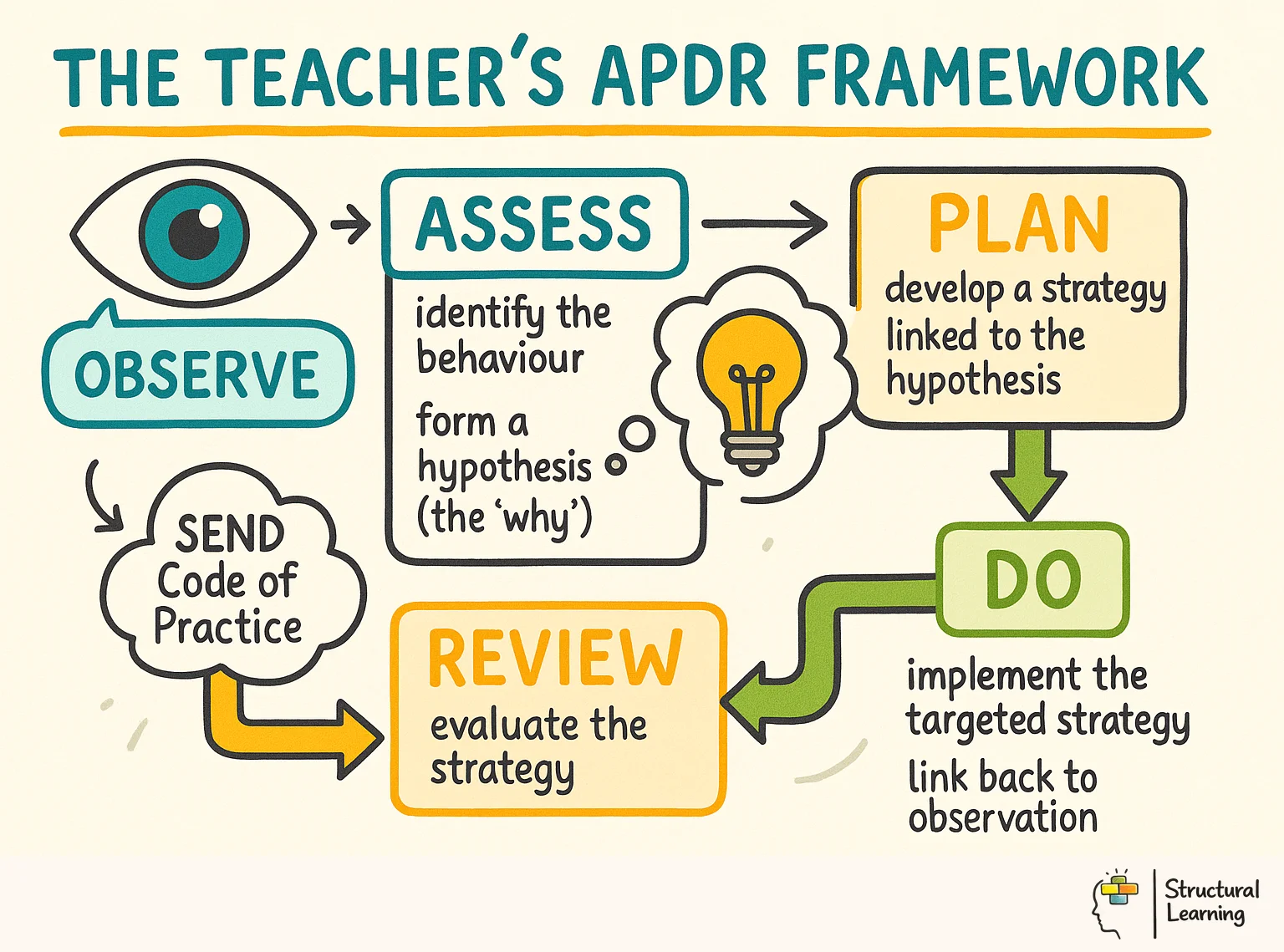
The matrix helps record your Assess-Plan-Do-Review cycle; download the PDF. This PDF gives a clear record of observations. This record assists referrals to educational psychology or CAMHS.
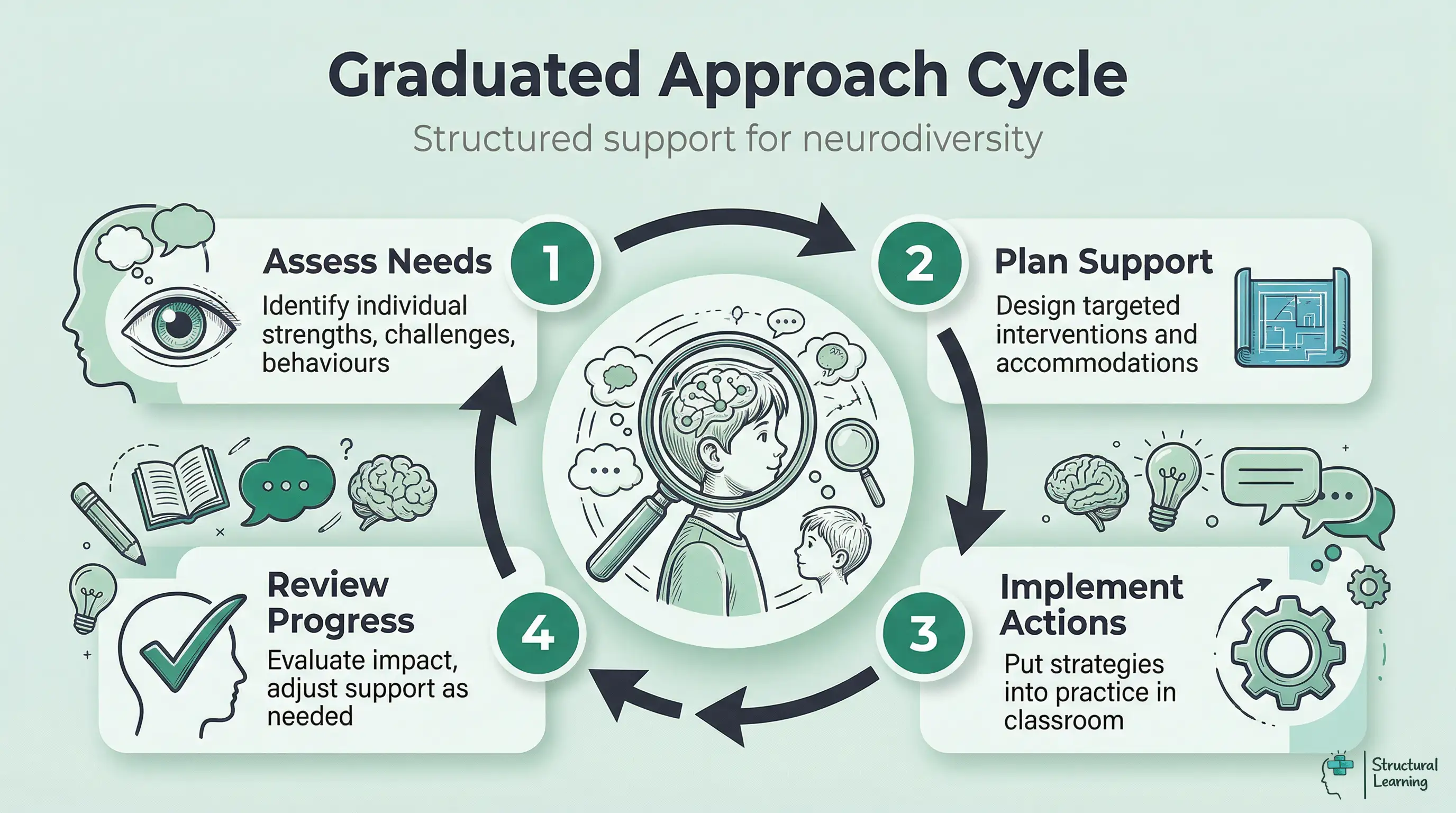
The SEND Code of Practice (DfE, 2015) requires schools to follow a Graduated Approach before seeking external assessment. The symptom overlap framework fits directly into this cycle. Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
Refer to educational psychology or CAMHS when:
The Matrix assessment data helps with learner referrals. Educational psychologists value structured data because it can support faster assessments (Frederickson & Cline, 2015). This strengthens your case when you work with external agencies.
Symptom overlap becomes even more complex when masking is considered. Autistic girls are diagnosed on average 1.8 years later than autistic boys (Begeer et al., 2013), partly because they learn to copy the social behaviours of neurotypical peers. A girl who appears socially competent in class but experiences daily meltdowns at home may be masking her autism. If the SENCO only observes school behaviour, the presentation may look like anxiety or, in some cases, ODD.
ADHD in girls often differs from typical hyperactive boys. Girls often show inattention, like daydreaming, rather than acting out (Hinshaw et al., 2022). Teachers may miss this until secondary school. Academic pressures increase and coping strategies stop working.
The matrix helps compare a learner's school and home behaviours. A big difference between settings can suggest masking (Attwood, 2006; Lai et al., 2017). This discrepancy can provide key insight (Gould & Ashton-Smith, 2011; Gillberg et al., 2014).
This week: Choose one learner whose presentation puzzles you. Use the Symptom Overlap Matrix to compare the two or three conditions you suspect. Download the PDF and file it in the learner's SEND record.
This half-term: Share the matrix with your teaching staff during a SEND twilight session. Walk through the six domains and discuss how to distinguish overlapping presentations using the "how to tell the difference" guidance.
This term: Audit your current SEND register. For learners with a single identified need, check whether their classroom presentation suggests co-occurring conditions that may have been overlooked. The SEND Code of Practice encourages schools to review and update assessments as new information emerges.
The conditions in this article are not separate boxes; they are overlapping spectra, so learners need professionals who can make sense of complex classroom patterns. Since the pandemic, schools also need to tell neurodevelopmental demand avoidance apart from EBSA, school distress, masking exhaustion and neurodivergent burnout; attendance data alone will not show which barrier is operating (Connolly et al., 2023). Vygotsky (1978) supports guided social learning, and Karpicke (2008) shows why retrieval strengthens memory, but direct prompting, public questioning or timed quizzes can feel like demands to some neurodivergent learners. The Symptom Overlap Matrix gives a clear framework for moving from "I think this is ADHD" to "here is the systematic evidence for what I observe, and here is what distinguishes it from the alternatives."
Autistic learners often benefit from predictability, clear routines and reduced sensory uncertainty (Attwood, 2006). Learners with a PDA profile may experience those same routines as imposed control when they are presented as non-negotiable demands. The practical difference is the route into the task: autism support often starts with clarity, while PDA support starts with autonomy, indirect language and genuine choice (Christie et al., 2011; O'Nions et al., 2014; Green et al., 2018).
Start with predictable routines, then build in flexible entry points. Autistic learners often need clear expectations and sensory preparation (Hill, 2004), while learners with ADHD often need movement, novelty, external organisation and shorter task chunks (Barkley, 2015). For AuDHD learners, the aim is not more rules; it is a stable environment with flexible routes through the work, such as standing to write, choosing task order or using a visual timer without public pressure.
Getting the profile wrong can damage behaviour plans and make distress worse. ODD describes a pattern of angry, argumentative or vindictive behaviour, while demand avoidance is usually understood as anxiety linked to a perceived loss of control. This difference also matters for equity: research on autism and ADHD identification shows that Black, minoritised and low-income learners are more likely to be missed, diagnosed later, or sent through behaviour labels before developmental need is recognised (Mandell et al., 2009; Morgan et al., 2013). Before treating refusal as defiance, use indirect language, negotiation, sensory review and family evidence (Christie et al., 2011; Gillberg, 2014).
The evidence points to co-occurrence, not strict separation. Leitner (2014) reported high rates of ADHD in autistic populations. Rommelse et al. (2010) found shared genetic and environmental risk between ADHD and ASD. For schools, this means one label should not end the assessment: attention, sensory regulation, social communication and executive function all need to be reviewed together.
Using typical behaviour policies can worsen anxiety for learners with demand avoidance. A zero-tolerance response treats refusal as wilful misconduct, so the school increases sanctions at the same point the learner's sense of threat is rising. That pattern can lead to repeated exclusions, weak reasonable-adjustment evidence and avoidable complaints. Sanctions and rewards may escalate distress in PDA profiles, so teachers should reduce direct commands, use indirect language, offer real choices and record what lowers arousal (Christie et al., 2011; Gillberg, 2014; Green et al., 2018).
| APDR Stage | What You Do | Tool to Use |
|---|---|---|
| Assess | Structured classroom observation across 6 domains for 2-4 weeks | Symptom Overlap Matrix (above) |
| Plan | Identify likely conditions and plan targeted classroom adjustments | Differentiation guidance from the matrix, condition-specific strategy cards |
| Do | Implement adjustments for 6-8 weeks, tracking frequency and intensity of target behaviours | Behaviour tracking sheets, ABC charts |
| Review | Compare pre- and post-intervention data; decide whether to continue, adjust, or escalate | Symptom Overlap Matrix re-assessment + PDF comparison |
The main limit is diagnostic certainty. PDA is not a separate diagnostic category in DSM-5-TR or ICD-11. Green et al. (2018) describe it as symptoms rather than a syndrome. Kildahl et al. (2021) reviewed the child and adolescent evidence and found small, mixed-method studies, heavy reliance on parent report, circular definitions based on Newson's original criteria, and limited attention to other explanations such as anxiety, trauma or sensory overload.
A second critique focuses on language and power. Milton and Woods (2018) argue that "pathological" can present autistic resistance, masking and self-advocacy as disorder. These behaviours may instead be responses to demands that feel unsafe.
This matters culturally because the same classroom behaviour may be read differently by race, gender, social class and parental confidence. Research on autism and ADHD identification shows persistent inequities in who receives protective developmental explanations and who receives punitive behaviour labels (Mandell et al., 2009; Morgan et al., 2013).
Broad learning theory also has limits: Vygotsky (1978) helps teachers plan social scaffolding, and Karpicke (2008) supports retrieval practice. However, neither framework was built around sensory overload, demand avoidance or neurodivergent burnout. If schools use prompts, public questioning and repeated recall too rigidly, they can increase threat rather than learning. This comparison still has practical value: it helps schools replace blame with observation and adapt support while staying honest about diagnostic uncertainty.
Karpicke, J. (2008). The critical importance of retrieval for learning.
Vygotsky, L. (1978). Mind in society: The development of higher psychological processes.
Use this free, interactive tool to compare overlapping traits across ADHD, autism, PDA, ODD, and specific learning difficulties. No learner data is stored. Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
Compare shared and unique symptoms across conditions Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.

Select at least two conditions above to compare their symptoms side by side.

Learners with ADHD often have other issues too. These issues can include psychiatric problems (Brown et al., 2001). Medical conditions and learning difficulties are also common (DuPaul et al., 2011). Developmental Coordination Disorder may occur with ADHD (Gillberg, 2003).
92 citations
Leitner (2014)
Autism and ADHD frequently co-occur. Researcher Names & Dates found 50-70% of autistic learners also have ADHD. This informs teacher understanding of overlapping needs in learners.
The Structure of Shared Genetic and Environmental Risk Factors for ADHD and ASD View study ↗
248 citations
Rommelse et al. (2010)
Twin studies (Landmark) show shared genes link ADHD and autism. This explains why these conditions often occur together in families and learners. Researchers found this overlap is common, not unusual.
Emotion Dysregulation in Autism Spectrum Disorder View study ↗
380 citations
Mazefsky et al. (2013)
Researchers show emotional dysregulation is common in autism and ADHD. This challenges the idea that meltdowns always mean ADHD. They offer ways to tell the difference. Use this to separate autism crises from ADHD impulsivity.
NIDCAP supports infant development (Als, 1982). It may help learners avoid later ADHD executive function issues. Als (1998) researched this possible link. Brazelton & Cramer's (1990) studies add to our understanding.
Foundational
Barkley (2012)
Pennington and Ozonoff (1996) made a core ADHD executive function model. It splits ADHD (inhibition problems) from autism (flexibility problems). This clarifies why learners face different planning and organisation issues.