Updated on
July 2, 2026
504 Plan for Anxiety: Accommodations for Teachers
Evidence-based accommodations for 504 plans addressing anxiety: scaffolded exposure frameworks, condition-specific strategies.


Updated on
July 2, 2026
Evidence-based accommodations for 504 plans addressing anxiety: scaffolded exposure frameworks, condition-specific strategies.
Anxiety-related need is a common and visible issue in American classrooms. The Centers for Disease Control and Prevention reports that 11% of children aged 3-17 had current, diagnosed anxiety in recent national data. For general education teachers, school counsellors and 504 coordinators, the practical question is not whether anxiety exists, but whether it substantially limits the student's access to learning, concentration, thinking, communication or participation at school.
Section 504 of the Rehabilitation Act protects students with disabilities from discrimination in federally funded education programmes. OCR guidance frames eligibility as an individual inquiry: the team asks whether a physical or mental impairment substantially limits one or more major life activities, including learning, thinking, concentrating or communicating. Anxiety may be relevant when it substantially limits access, but the plan should document the school impact and the accommodations needed for equal access.
Section 504 has a wide definition of disability. Learners qualify if a physical or mental problem greatly limits life activities. The Office for Civil Rights (OCR) enforces Section 504. They say key life activities include learning, concentrating, and thinking. OCR also lists communicating and self-care. Anxiety can impact all these areas.
The critical word is 'substantially.' A student who feels nervous before a test does not qualify. A student may qualify if their anxiety causes them to freeze during tests, miss important class time due to avoidance, or struggle to complete work in normal classroom conditions. The team's job is to gather evidence of how anxiety functions in the school environment, not simply to confirm that a diagnosis exists.
Schools gather information from psychologists, teachers and parents. Attendance, grades, work completion and adaptive behaviour can also provide data for review. OCR's Section 504 resource guide says teams may consider medical diagnoses or medical assessments, but eligibility still turns on the student's functional limitation and educational need, not on a diagnosis label alone.
Teachers should note attendance patterns, requests to leave, underperformance, reassurance-seeking and distress linked to specific tasks. Share these observations with the counsellor or 504 coordinator. OCR guidance allows teams to use teacher recommendations and adaptive behaviour data, so classroom evidence matters.
Anxiety shows itself in many ways. Good accommodations should fit the learner's functional profile rather than a generic anxiety list. That means connecting the trigger, the school activity and the intended access outcome, then checking whether the support is helping over time.
Generalised anxiety often involves persistent worry across situations, intolerance of uncertainty and repeated reassurance-seeking. In school, that can look like difficulty starting open tasks, repeated deadline questions or physical complaints before demanding work. Treat these observations as a functional hypothesis for the school team, not a classroom diagnosis (Rapee, Schniering and Hudson, 2009).
Social anxiety causes fear of scrutiny (Rapee et al., 2009). Class triggers include answering questions and group work. Learners may view neutral expressions as disapproval. Avoidance presents as refusal or illness.
Separation anxiety can involve distress about leaving caregivers or being away from home. Older learners may avoid school, repeatedly seek reassurance or ask to contact home during the day. The school task is to preserve access while helping the learner tolerate separation gradually and predictably (Rapee, Schniering and Hudson, 2009).
Selective mutism is usually understood as an anxiety-related difficulty in which a learner can speak in some settings but not in others, often including school. ASHA and clinical reviews stress careful assessment, collaboration and gradual communication goals rather than treating silence as defiance (Viana, Beidel and Rabian, 2009).
Test anxiety can affect attention and working memory during assessments. Eysenck et al. (2007) argue that anxiety can reduce the efficiency of attentional control, which helps explain why a prepared learner may struggle to retrieve or organise knowledge under pressure.
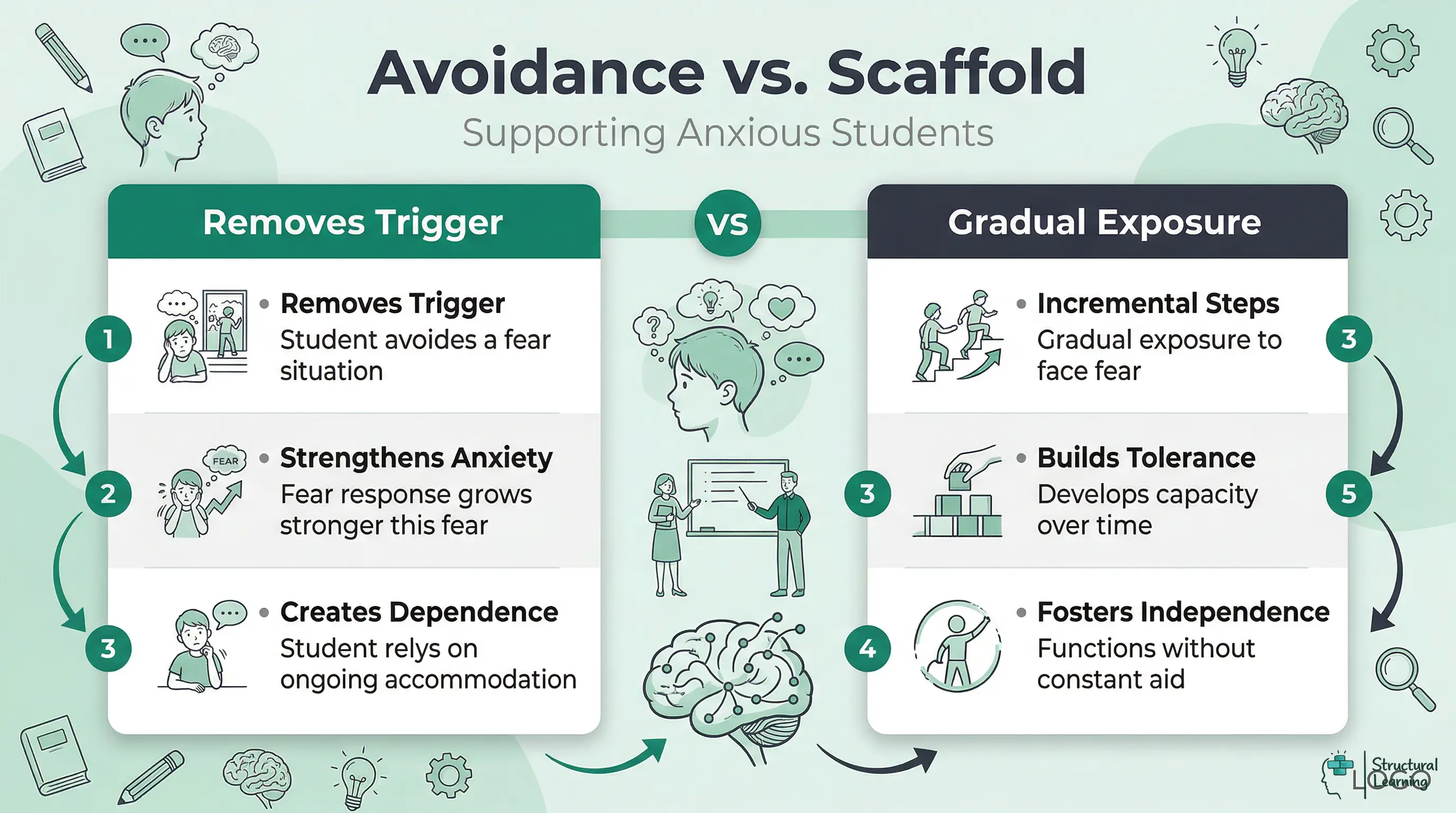
The most common 504 accommodations for anxiety follow an avoidance logic. The student finds presentations distressing, so the plan states they are not required to present. The student becomes overwhelmed during timed tests, so the plan removes time limits entirely. The student avoids group work, so the plan permits individual completion of all group tasks. These accommodations feel compassionate, and in the short term they work: the student's distress decreases when the trigger is removed.
The problem is what happens over months and years. Evidence reviews of child anxiety treatments identify CBT and exposure-oriented approaches as among the better supported psychosocial treatments for phobic and anxiety disorders (Silverman, Pina and Viswesvaran, 2008). A school 504 Plan should not try to run therapy, but it should avoid making permanent avoidance the only documented route to access.
Rapee, Schniering and Hudson (2009) describe exposure as a central component of evidence-based anxiety treatment, and Mychailyszyn et al. (2012) found that school-based CBT interventions can reduce anxiety symptoms. The classroom translation should be cautious: reduce access barriers, coordinate with qualified professionals where possible and build gradual participation steps that do not overwhelm the learner.
504 Plans that only remove triggers can reduce immediate distress while leaving the learner without a route back into the activity. That is not the same as saying every learner should be pushed into severe distress. The safer aim is access plus planned review: protect participation now, then ask whether the accommodation is building independence or becoming a permanent avoidance pathway.
Teachers should not improvise exposure work or deliberately push learners into severe distress. Within an agreed plan, however, accommodations can reduce safety behaviours gradually and increase participation step by step. Craske et al. (2014) emphasise exposure as new learning rather than simple distress tolerance, which is why school steps should be small, observable and reviewed.
The 'Anxiety-to-Access Bridge' reframes every avoidance accommodation as a graduated sequence. Instead of writing what a student does not have to do, the 504 team writes what the student will do at each stage. They include clear criteria for moving to the next stage. This approach keeps the student in the curriculum while building tolerance systematically.
The framework works by identifying the anxiety trigger and establishing the long-term target behaviour. This means what the student should be able to do without accommodation. Then it creates steps that connect where the student is now to where the team wants them to be. Each step includes a support that fades at the next step.
Long-term target: Student presents independently to the full class.
Step 1: Student presents to the teacher only, after school or during a free period, with notes permitted.
Step 2: Student presents to the teacher and one trusted peer, with notes permitted.
Step 3: Student submits a pre-recorded video presentation, reviewed only by the teacher.
Step 4: Student presents live to a small group of three to four students, with notes permitted.
Step 5: Student presents to the full class with notes permitted.
Step 6: Student presents to the full class without notes.
Learners progress after meeting the step criterion set by the team. The 504 team should record the current step, the evidence used to move on and the next scheduled review point. If the learner stalls, the team should revise the support rather than simply leaving the sequence unchanged.
Long-term target: Student completes assessments under standard time conditions.
Step 1: Extended time (double time) with a separate, quiet room.
Step 2: Extended time (1.5x) with a separate, quiet room.
Step 3: Standard time with a separate, quiet room.
Step 4: Standard time in the regular classroom.
Extended time can be an appropriate access support, but it should not be written as an unreviewed default. OCR's Section 504 resource guide expects teams to use evaluation information and placement data, so the plan should specify what evidence will be reviewed before changing the level of support. If anxiety is the barrier, the team should ask whether time, setting, instruction clarity, pacing support or clinical input is the relevant need.
Long-term target: Student participates in self-selected groups, then randomly assigned groups.
Step 1: Student completes the task individually, with the teacher noting which group task elements they demonstrate solo.
Step 2: Student works in a pair with a teacher-selected partner.
Step 3: Student works in a group of three, with a pre-assigned role that provides structure.
Step 4: Student works in a group of four with a rotating role.
Step 5: Student participates in randomly assigned groups.
Long-term target: Student transitions between environments and activities independently.
Step 1: Student receives a written schedule at the start of each day and a verbal one-minute warning before transitions.
Step 2: Student receives only a written schedule, without verbal warnings.
Step 3: Student uses the classroom schedule posted on the board, without personal copies.
Long-term target: Student completes written assignments under standard conditions.
Step 1: Student submits bullet-point outline, assessed for comprehension; no prose required.
Step 2: Student submits a partial draft, with teacher feedback before final submission.
Step 3: Student submits a complete first draft for feedback, with revision opportunity.
Step 4: Student submits a final draft only, under standard conditions.
The key principle across all triggers is that every step is a real step toward independence, not a holding position. If a student stays at Step 2 for a whole semester without progress, the 504 team must check three things. Is the scaffold working? Is the student getting CBT support outside school? Do they need more intensive support?
Anxiety affects how learners engage, so plan support from observed barriers rather than generic accommodation menus. The team should name the trigger, the access barrier, the support and the evidence that will show whether the support is working.
Accommodations can help learners with generalised anxiety when uncertainty and repeated worry block school tasks. Reduce unnecessary uncertainty, make task demands explicit and set limits around reassurance-seeking so the support improves access without becoming another avoidance routine (Rapee, Schniering and Hudson, 2009).
Written schedule and advance notice of changes. Provide a written schedule at the start of each day, and give at least 24 hours' notice when the schedule will change. This does not mean protecting the student from all changes; it means giving them time to process change before it arrives. The goal is reducing surprise, not preventing flexibility.
Clarification without penalty. Students with GAD need to know that seeking clarification is permitted and will not mark them out as incompetent. A brief classroom norm, "you can ask me to rephrase anything", removes the social cost of seeking reassurance. Do not, however, allow unlimited reassurance-seeking, as this is its own form of avoidance. One clarification per task is a reasonable limit.
Reduced assignment length in the short term. When GAD is causing significant impairment to task initiation, reducing the length of written tasks for a defined period while the student works with a therapist allows them to maintain curriculum access. This should be documented with a clear review date, not written as a permanent modification.
Flexible seating helps learners. Seating near exits or away from busy spaces lowers anxiety (GAD) that learners bring to lessons. This simple change costs nothing instructionally.
Social anxiety is often organised around fear of negative judgement (Rapee and Heimberg, 1997). Accommodations should reduce unnecessary public evaluation while still creating a gradual route towards contribution, because CBT and exposure-oriented treatments have evidence for youth anxiety (Silverman, Pina and Viswesvaran, 2008).
Pre-teach content before class. Give learners the discussion question the day before. Learners knowing their contribution reduces evaluation anxiety. This is useful for all learners needing processing time.
Cold-calling can increase learner anxiety when public evaluation is the trigger, so use planned participation routes. Learners can use hand signals, mini-whiteboards, exit tickets or prepared responses while the plan builds tolerated exposure. The aim is contribution with a lower initial social cost, not permanent invisibility.
Partner work before group work. Never assign a socially anxious student directly to a group of four or five. The scaffolded exposure framework applies: begin with a known partner, then a triad, then a larger group.
Consider learners' anxieties about grades. Return assessed work face down or through a private digital route when public comparison is a trigger. This is a low-cost access support, but the team should still review whether the learner is building tolerance for ordinary feedback over time.
Test anxiety mainly affects attention and working memory during tests. Eysenck et al. (2007) explain why worry can consume cognitive resources needed for problem solving. School-based CBT evidence also suggests that structured anxiety interventions can help some learners, but accommodation decisions still need individual review rather than a one-size-fits-all room change.
Extended time in a separate room. This combination addresses two problems. Extended time makes up for the slower thinking caused by anxiety. A separate room reduces social pressure that keeps worry going during a test. Neither accommodation is permanent in a scaffolded plan.
Teach a pre-assessment routine. Work with the counsellor to establish a short routine the student uses before every test: three slow breaths, two minutes of reviewing notes they know well, a single self-instruction cue such as "start with what I know." This addresses the cognitive mechanism directly and is something the student carries forward without the accommodation.
Read instructions aloud. Some students feel most anxious when reading test instructions. Reading instructions aloud or giving them in advance reduces confusion that can lead to panic.
Access to a familiar adult during the assessment. For students with high test anxiety, knowing that a familiar adult is in the room or accessible reduces physiological arousal. Over time, this access is faded: the adult is visible but not in the room, then available on request only, then not present at all.
For separation anxiety, the team should usually build tolerance for separation rather than permit unlimited contact with home. The exact step size depends on the learner's profile, family context and any clinical plan. In school, the practical aim is predictable reassurance that fades as the learner copes for longer periods.
One brief check-in call per day, at a fixed time. Not on demand. A student permitted to call home whenever distressed learns that distress produces contact, which maintains the separation anxiety. One call, timed, gives the student something to anticipate and reduces the unpredictability of separation. The frequency fades across the year.
A trusted adult the student can visit briefly. A specific adult, not "any available adult," reduces the student's anxiety about who to find in a moment of distress. The visit is brief (two to three minutes) and purposeful: the student checks in, uses a grounding strategy, and returns to class. This is not a sanctuary to wait in.
Visual structure for the school day. A printed schedule showing how the day breaks into segments, with an end time circled, gives separation-anxious students a concrete end point. "School ends at 3:15" is less anxiety-provoking than a formless day of unknown length.
Work with speech-language pathologists and mental-health professionals on selective mutism plans. ASHA describes the role of speech-language assessment and support, while selective mutism treatment resources emphasise gradual increases in communication across people and settings. School accommodations should match that planned progression.
Learners can sometimes show knowledge by writing, drawing, pointing or using carefully chosen communication supports while the communication plan is active. Record these formats as temporary access routes with review criteria, because the long-term goal is broader communication rather than permanent replacement of speech.
Forcing speech is risky when the learner has selective mutism. Avoid cold-calling or public pressure unless it is explicitly part of a specialist plan. Gradual communication goals, stimulus fading and reinforcement for small communication steps are more consistent with the selective mutism evidence base.
Slide talk before voice talk. Begin with the student communicating only with the teacher, in private. As comfort increases, the teacher introduces a second adult, then a peer. The first vocal communication the student produces is often a whisper in a one-to-one setting. That moment, however small, is a clinical and educational milestone.
A well-written 504 Plan for anxiety has six components. Vague language in any component creates implementation problems at the classroom level.
Use functional language rather than a diagnosis-only statement. For example: "Anxiety substantially limits this learner's ability to concentrate, communicate and participate in specified school activities. Section 504 accommodations are provided to give equal access while the team reviews progress and functional impact."
If timed tests are affected, state the school evidence directly: "During timed assessments, anxiety-related worry reduces this learner's ability to organise and retrieve knowledge under standard conditions." Eysenck et al. (2007) support the general anxiety-and-attention mechanism, but the team still needs local assessment data to justify the specific accommodation.
Specific accommodations with duration or review criteria. Write what the accommodation is, when it applies, and what the criterion for review is. "Student will receive 100% extended time for all assessments in a separate, quiet room for the first 12 weeks of the school year. At the 12-week review, the team will assess whether time can be reduced to 50% extended, based on assessment performance data and teacher observation."
Assign accommodation duties clearly. For example, the classroom teacher implements the agreed assessment setting, the counsellor or 504 coordinator monitors the presentation sequence and the team reviews progress at the scheduled checkpoint. Clear ownership prevents informal drift.
Review schedule. Anxiety 504 Plans should be reviewed more frequently than the standard annual review, particularly in the first year. Six-week reviews allow the team to track whether the scaffolded exposure plan is moving and to adjust if progress has stalled.
Shared understanding of the plan's goal matters. Every plan should include a statement of intent: "The goal of this plan is to build the student's capacity to access learning with reduced support over time. Accommodations will be reviewed and faded when evidence shows the student can access the activity with less support." This keeps the expectation clear for staff, families and the student.
Do not import accommodation language from another disability category unless it fits this learner's anxiety-related access barrier. The team should write supports that match the observed school function: presentation anxiety, test anxiety, separation distress, selective mutism, avoidance of group work or another defined barrier.
You did not write the 504 Plan. You use it, every day, in every lesson, and your implementation quality determines whether it works.
| Anxiety Trigger | Avoidance Accommodation (Common) | Scaffolded Exposure Accommodation (Evidence-Based) |
|---|---|---|
| Oral presentations | Student is exempt from all presentations | Student follows a 6-step sequence from teacher-only audience to full class; movement criteria defined |
| Timed assessments | Student receives unlimited time, indefinitely | Student begins at double time; plan includes a graduated reduction schedule reviewed at each 6-week meeting |
| Group work | Student completes all group tasks individually | Student begins in paired work with a teacher-selected partner; steps toward randomly assigned groups of four |
| Transitions between classes | Student given a pass to leave class early to avoid crowded hallways at all times | Student uses early pass for three weeks, then transitions two minutes early, then one minute early, then at standard time |
| New activities or tasks | Teacher previews all new tasks privately before the class session indefinitely | Teacher provides 48-hour preview for first three weeks, then 24-hour preview, then end-of-lesson preview for next day only |
| Written assignments under pressure | Student exempt from in-class writing; submits all work as take-home | Student begins with bullet outlines in class; builds to partial drafts; reaches full in-class drafting by agreed date |
| Speaking on the phone or to unfamiliar adults | Student communicates only through email or written notes; phone calls and verbal adult communication not required | Student practises scripted exchanges with familiar adults; advances to unscripted exchanges; then to brief contact with unfamiliar adults |
| Lunchtime and unstructured social periods | Student permitted to eat lunch in a separate room alone every day | Student begins lunch in small group (two others) with a counsellor present; advances to lunch in cafeteria with a pre-arranged peer; then to standard cafeteria lunch |
The most important thing you do is distinguish between a student using an accommodation and a student avoiding work. These look different. A student using extended time who is working steadily through the assessment is using their accommodation. A student using extended time who is sitting with their head down and producing nothing is avoiding. Both situations require different responses, and the 504 team needs your observations to make good decisions at reviews.
Learners with anxiety need consistent implementation. If advance notice, seating, assessment setting or participation scaffolds vary by teacher, the team loses both trust and useful data. Discuss inconsistent accommodation delivery in team meetings and correct it quickly.
Tell the counsellor if a learner's anxiety seems to worsen. Watch for more reassurance-seeking, new avoidance, or lesson-linked complaints. Note if accommodations fail to reduce their need. This data helps your team reviews.
Teachers should avoid undocumented accommodations, even when the intention is kind. Extra informal support can blur the graduated plan, distort review data and make it harder to know what is actually helping. If the written plan is insufficient, bring that evidence back to the team rather than expanding support independently.
Cognitive load theory can help you design lessons that reduce anxiety. Tasks with high load are harder when instructions are unclear (Sweller, 1988). Clear instructions and structure help all learners, especially those with anxiety (Paas et al., 2003; Chandler & Sweller, 1991).
Know the attention and executive demands of tasks. Anxiety may disrupt attentional control and make planning, switching or organising harder under pressure (Eysenck et al., 2007). Treat this as a reason to design clearer tasks and review evidence, not as a reason to assume laziness.
Chunking tasks and worked examples help all learners because they reduce unnecessary processing demands. Choice and processing time can also aid access when anxiety makes task initiation harder. These strategies are better supported by cognitive load theory than by the placeholder citations previously attached here (Sweller, 1988; Chandler and Sweller, 1991; Paas, Renkl and Sweller, 2003).
504 Plans provide accommodations and related aids or services needed for equal access; they are not a substitute for clinical treatment. If a learner needs therapeutic exposure, crisis planning or intensive mental-health support during the school day, the team should review whether the current 504 Plan is enough and whether other services or evaluations are required.
Request a fuller evaluation if attendance drops despite support, if the learner cannot access learning after a sustained review period, if anxiety requires significant adult support during the school day or if grades fall across subjects despite implemented accommodations. Bring attendance, work completion, assessment data and teacher observations to the meeting.
An IEP may include specially designed instruction and related services when the student qualifies under IDEA and those services are required for FAPE. That can include social-emotional instruction, counselling as a related service or a crisis plan, depending on the evaluation and local provision. Do not promise a service simply because anxiety is present; match the plan to eligibility and need.
It is useful to grasp the link between 504 Plans and MTSS. Some learners with anxiety have already received Tier 2 help such as small groups or counsellor support before a formal 504 Plan. If the learner does not respond after a sustained review period, the team may need Tier 3 support, an IDEA evaluation or referral to an outside provider, with appropriate consent and privacy safeguards.
If a student has an existing 504 Plan and their anxiety is worsening rather than improving, the team needs to meet, not wait for the annual review. Request a meeting, bring your observational data, and make the case that the current plan is not producing the intended outcome. If progress has stalled completely, see our guide on what to do when IEP progress stalls, which addresses the same fundamental question of what to do when a support plan is not working.
In England, schools do not create 504 Plans for learners with anxiety. The Equality Act 2010 means schools must make reasonable adjustments for learners with disabilities. Schools often address this through tiered support, such as differentiation (Tier 1). Small group work (Tier 2) and specialist support (Tier 3) follow.
UK education has two clear benefits. Teachers view many adjustments as teaching decisions, not a separate civil-rights document, and schools use a graduated assess-plan-do-review cycle. The Department for Education's SEND Code of Practice describes this graduated approach, while the Equality Actundefinedunderpins reasonable adjustments for disabled learners.
The lesson for US teachers and 504 coordinators is not that the formal 504 document is unnecessary. It is not. Students with anxiety need legal protection, clear documentation, and consistent implementation. But the 504 document should read like a teaching plan, not a liability checklist. The best 504 plans for anxiety feel like what a reflective teacher would naturally do for that student, written down with specificity and a review date. A growth mindset approach means viewing the 504 Plan as a working document that changes as the student grows. This is better than seeing it as a fixed entitlement. This approach brings it closer to the spirit of effective differentiation in both systems.
Every accommodation in a 504 Plan for anxiety should follow this structure: what, when, by whom, and what the review criterion is. The following template shows how to write accommodations that are specific enough to use and honest enough to improve.
Extended time template: "[Student] will receive [agreed percentage] additional time for specified assessments in [grade/year group]. Assessments will be completed in [room/location] to reduce distraction. At the scheduled review point, the team will consider whether the level of support should change based on assessment performance data and teacher observation notes from the previous grading period."
Presentation scaffold template: "[Student] is currently at Step [current step] of the oral presentation scaffold. The responsible adult for tracking progress through the scaffold is [name and role]. Progress to the next step requires [criterion]. The team will review progress at the scheduled review point."
Transition support template: "[Student] will receive a written schedule at the start of each school day and 24 hours' advance notice of changes. This accommodation will be reviewed at the scheduled review point with the goal of reducing to [end-of-day notice of the following day's schedule] when evidence shows the student can tolerate the change."
Participation scaffold template: "[Student] will use [agreed participation route] during whole-class questioning. The route will be reviewed at [scheduled review point] using teacher observations, student feedback and participation data. The team will consider the next step when the student can contribute reliably with the current support."
504 Plans give eligible students with disabilities the accommodations, aids or services needed for equal access to school. For anxiety, the team should document the functional limitation, the access barrier and the support that addresses it.
Teachers use scaffolded exposure by breaking intimidating tasks into smaller, manageable steps over time. For example, instead of excusing a student from public speaking entirely, the teacher might ask them to present to just the teacher first. The student then gradually progresses to presenting to a small peer group, and finally the whole class.
Graduated accommodations can protect access while building participation over time. The team starts with enough support for the learner to engage, then reviews whether the support can be reduced as tolerance and independence improve.
Research on anxiety treatment supports gradual, planned exposure rather than permanent avoidance. In school, that means carefully staged participation, not forcing distress or asking teachers to deliver therapy.
Common mistakes include writing permanent exemptions, copying generic accommodation lists, failing to review progress and allowing informal supports to replace the written plan. Stronger plans target a specific barrier and define how the team will know whether access is improving.
A medical diagnosis can be useful evidence, but OCR guidance frames Section 504 eligibility around whether an impairment substantially limits a major life activity. Teacher notes, attendance, grades, work completion and parent or clinical information can all help the team decide functional impact.
These sources replace placeholder citations and over-specific claims that could not be verified. They should be used cautiously: clinical treatment evidence supports the general principle of graduated exposure and CBT, while Section 504 sources govern school access and accommodation decisions.
U.S. Department of Education, Office for Civil Rights. Frequently Asked Questions: Section 504 Free Appropriate Public Education. View official FAQ
Use this for Section 504 eligibility, major life activities, FAPE and the requirement for an individual inquiry.
U.S. Department of Education, Office for Civil Rights (2016). Parent and Educator Resource Guide to Section 504 in Public Elementary and Secondary Schools. View OCR guide
Use this for evaluation sources, knowledgeable team decision-making and data-based placement or accommodation decisions.
Centers for Disease Control and Prevention. Data and Statistics on Children's Mental Health. View CDC data
Use this for current U.S. child mental-health prevalence, including diagnosed anxiety among children aged 3-17.
Rapee, R. M., Schniering, C. A. and Hudson, J. L. (2009). Anxiety Disorders During Childhood and Adolescence: Origins and Treatment. View DOI record
Use this for broad child and adolescent anxiety development and treatment principles, not for a specific school-legal rule.
Silverman, W. K., Pina, A. A. and Viswesvaran, C. (2008). Evidence-Based Psychosocial Treatments for Phobic and Anxiety Disorders in Children and Adolescents. View DOI record
Use this for the evidence base around CBT and exposure-oriented treatments for child anxiety. Do not use it to claim that a 504 Plan is a clinical intervention.
Mychailyszyn, M. P., Brodman, D. M., Read, K. L. and Kendall, P. C. (2012). Cognitive-behavioral School-based Interventions for Anxious and Depressed Youth: A Meta-analysis of Outcomes. View DOI record
Use this for school-based CBT outcomes in anxious and depressed youth, with cautious translation into school support planning.
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T. D. and Vervliet, B. (2014). Maximizing Exposure Therapy: An Inhibitory Learning Approach. View DOI record
Use this for the clinical principle that exposure should build new learning and reduce reliance on safety behaviours; school staff should apply this only within appropriate plans and boundaries.
Eysenck, M. W., Derakshan, N., Santos, R. and Calvo, M. G. (2007). Anxiety and Cognitive Performance: Attentional Control Theory. View DOI record
Use this for anxiety, attention and cognitive performance claims, especially test-anxiety and working-memory framing.
Viana, A. G., Beidel, D. C. and Rabian, B. (2009). Selective Mutism: A Review and Integration of the Last 15 Years. View DOI record
Use this for selective mutism as an anxiety-related condition and for the need for careful assessment and intervention planning.
American Speech-Language-Hearing Association. Selective Mutism. View ASHA guidance
Use this for speech-language evaluation and school support roles in selective mutism.
Department for Education and Department of Health and Social Care. SEND Code of Practice: 0 to 25 Years. View GOV.UK guidance
Use this only for the England comparison: graduated assess-plan-do-review support, not U.S. Section 504 eligibility.
American Speech-Language-Hearing Association. Selective mutism.
Centers for Disease Control and Prevention. Data and statistics on children's mental health.
Chandler, P. and Sweller, J. (1991). Cognitive load theory and the format of instruction. Cognition and Instruction, 8(4), 293-332.
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T. D. and Vervliet, B. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10-23.
Department for Education and Department of Health and Social Care. SEND code of practice: 0 to 25 years.
Eysenck, M. W., Derakshan, N., Santos, R. and Calvo, M. G. (2007). Anxiety and cognitive performance: Attentional control theory. Emotion, 7(2), 336-353.
Mychailyszyn, M. P., Brodman, D. M., Read, K. L. and Kendall, P. C. (2012). Cognitive-behavioral school-based interventions for anxious and depressed youth: A meta-analysis of outcomes. Clinical Psychology: Science and Practice, 19(2), 129-153.
Paas, F., Renkl, A. and Sweller, J. (2003). Cognitive load theory and instructional design: Recent developments. Educational Psychologist, 38(1), 1-4.
Rapee, R. M. and Heimberg, R. G. (1997). A cognitive-behavioral model of anxiety in social phobia. Behaviour Research and Therapy, 35(8), 741-756.
Rapee, R. M., Schniering, C. A. and Hudson, J. L. (2009). Anxiety disorders during childhood and adolescence: Origins and treatment. Annual Review of Clinical Psychology, 5, 311-341.
Silverman, W. K., Pina, A. A. and Viswesvaran, C. (2008). Evidence-based psychosocial treatments for phobic and anxiety disorders in children and adolescents. Journal of Clinical Child & Adolescent Psychology, 37(1), 105-130.
Sweller, J. (1988). Cognitive load during problem solving: Effects on learning. Cognitive Science, 12(2), 257-285.
U.S. Department of Education, Office for Civil Rights. Frequently asked questions: Section 504 free appropriate public education.
U.S. Department of Education, Office for Civil Rights. Parent and educator resource guide to Section 504 in public elementary and secondary schools.
Viana, A. G., Beidel, D. C. and Rabian, B. (2009). Selective mutism: A review and integration of the last 15 years. Clinical Psychology Review, 29(1), 57-67.