Updated on
July 2, 2026
Tests for Dyspraxia
Learn to identify dyspraxia signs in your classroom and discover which assessment pathways lead to proper diagnosis and support for struggling learners.


Updated on
July 2, 2026
Learn to identify dyspraxia signs in your classroom and discover which assessment pathways lead to proper diagnosis and support for struggling learners.
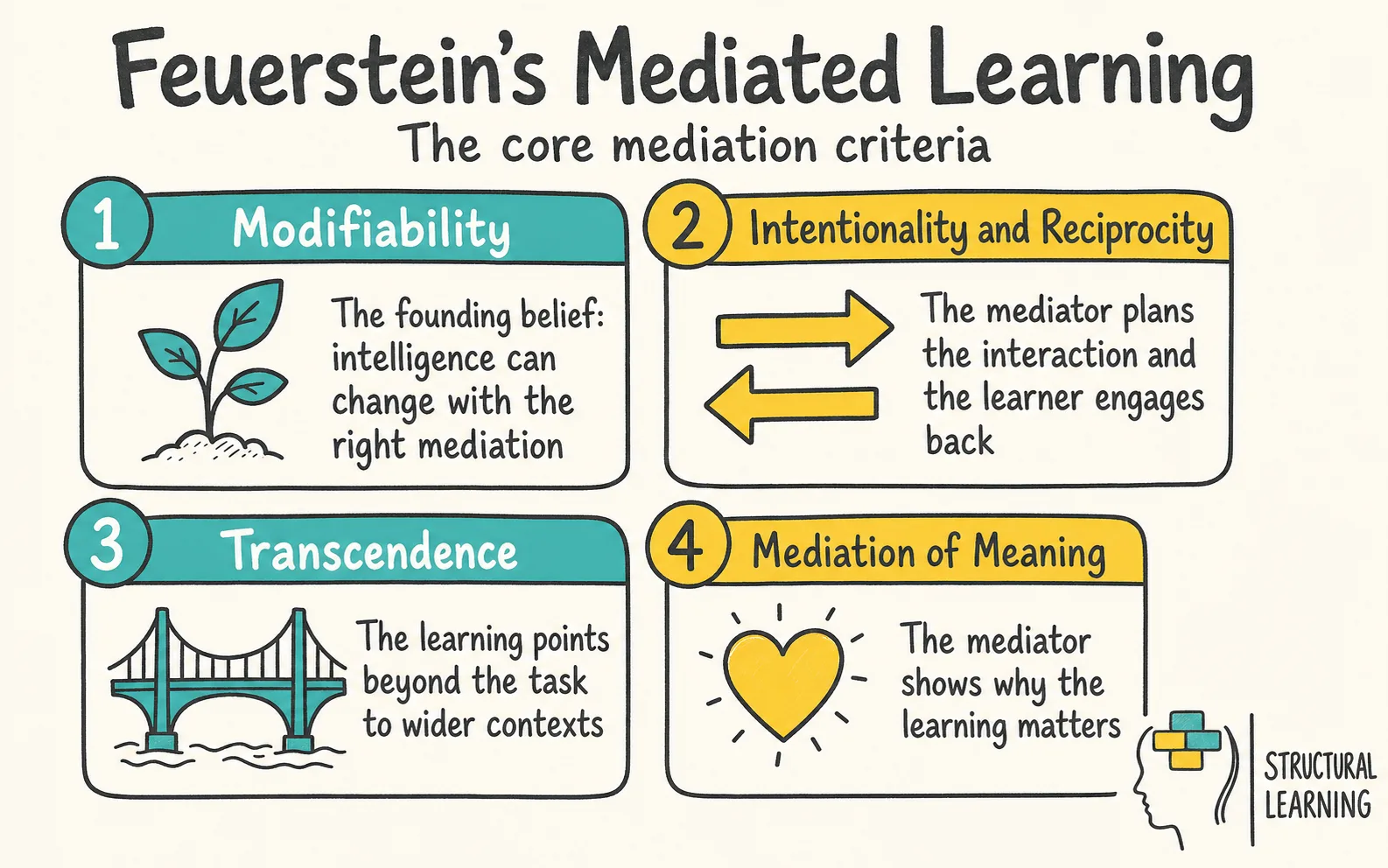
Tests for Dyspraxia explains how teachers and clinicians spot signs of Developmental Coordination Disorder, the clinical term often used for dyspraxia. DCD is a neurodevelopmental condition. This means a learner's motor coordination is below the level expected for their age and chances to practise. The difficulty also affects schoolwork, self-care or play (Blank et al., 2019).
In class, this may look like a learner who understands a science investigation but struggles with the practical tasks around it. They may not be able to copy the results table, handle scissors safely, organise PE movements or finish written work before the lesson moves on. Formal assessment can help, but support should not wait for a diagnosis. While specialist assessment is being arranged, teachers can record patterns, reduce unnecessary handwriting load, adjust equipment and use assistive technology.
Many UK families and teachers use dyspraxia to mean Developmental Coordination Disorder, or DCD. However, the terms are not always exact synonyms. DCD is the formal clinical term for a neurodevelopmental condition that affects the learning and use of coordinated motor skills, while dyspraxia can also mean narrower difficulties with praxis, or planning skilled movement (NHS, 2023; Blank et al., 2019). A learner may know the answer in maths but still lose marks because aligning numbers, copying diagrams and controlling pencil pressure use up working memory (Subara-Zukic et al., 2022).
Developmental Coordination Disorder affects around 5-6% of school-age children (American Psychiatric Association, 2022; Blank et al., 2019). This means most classes will have one or two learners with DCD. Boys get diagnosed more often than girls.
, 2020). Girls' DCD often appears as avoidance or quietness. This differs from the clumsiness prompting boys' referrals (Kirby et al., 2011).
Dyspraxia is usually long term, but support can reduce its impact. Teachers should not wait for a formal diagnosis before they act. While a referral is being considered, they can start to gather classroom evidence, make reasonable adjustments and review the SEN Support plan in line with the SEND Code of Practice and the SEND and AP Improvement Plan (Department for Education and Department of Health, 2015; Department for Education, 2023; SASC, 2025).
Developmental Coordination Disorder often occurs with needs like dyslexia (Nicolson & Fawcett, 2007). A learner with one condition may also have DCD (Kirby et al., 2008)., 2018).
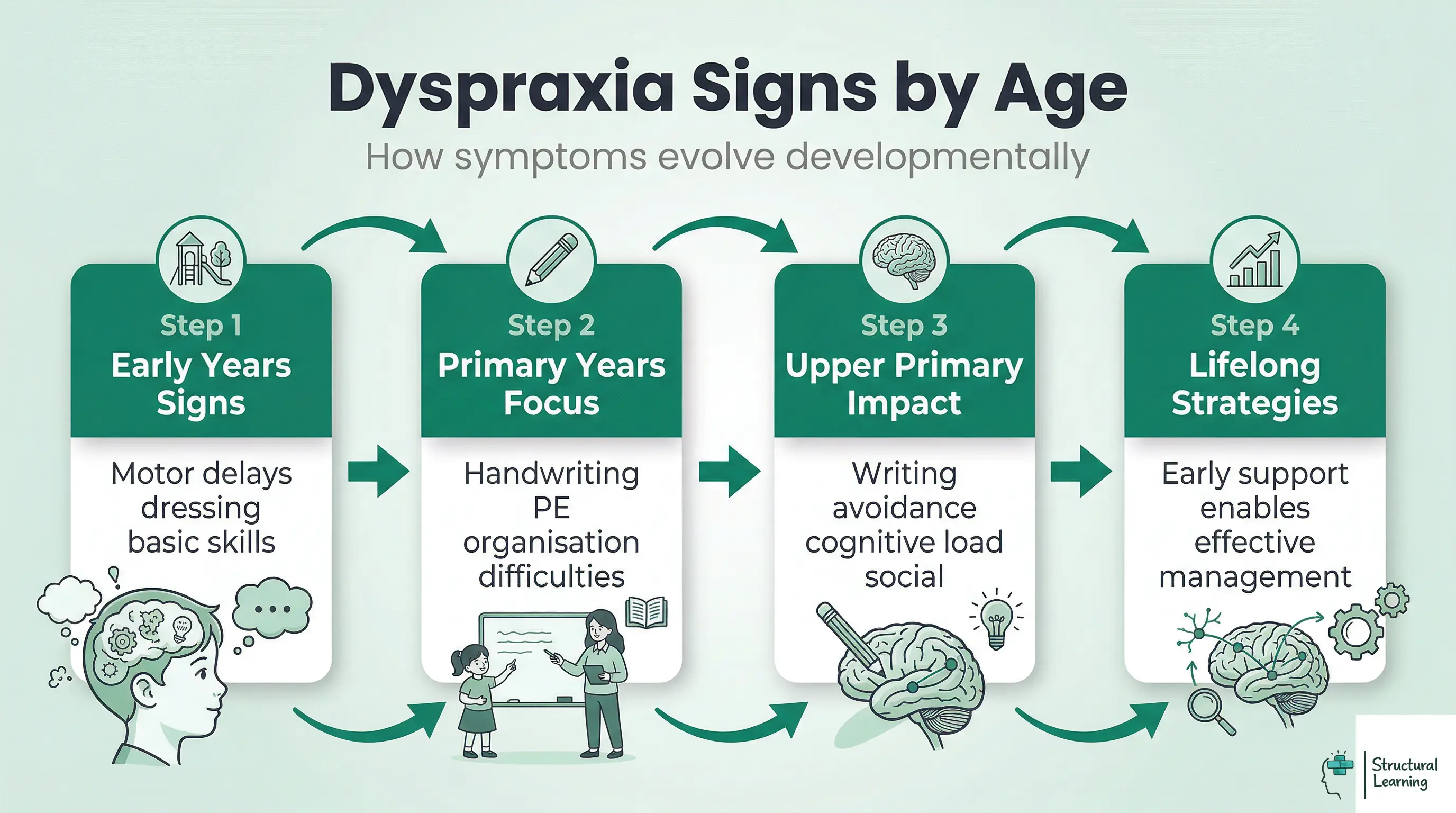
Teachers should look for signs that fit the learner's age and key stage (Kirby, 2011). Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
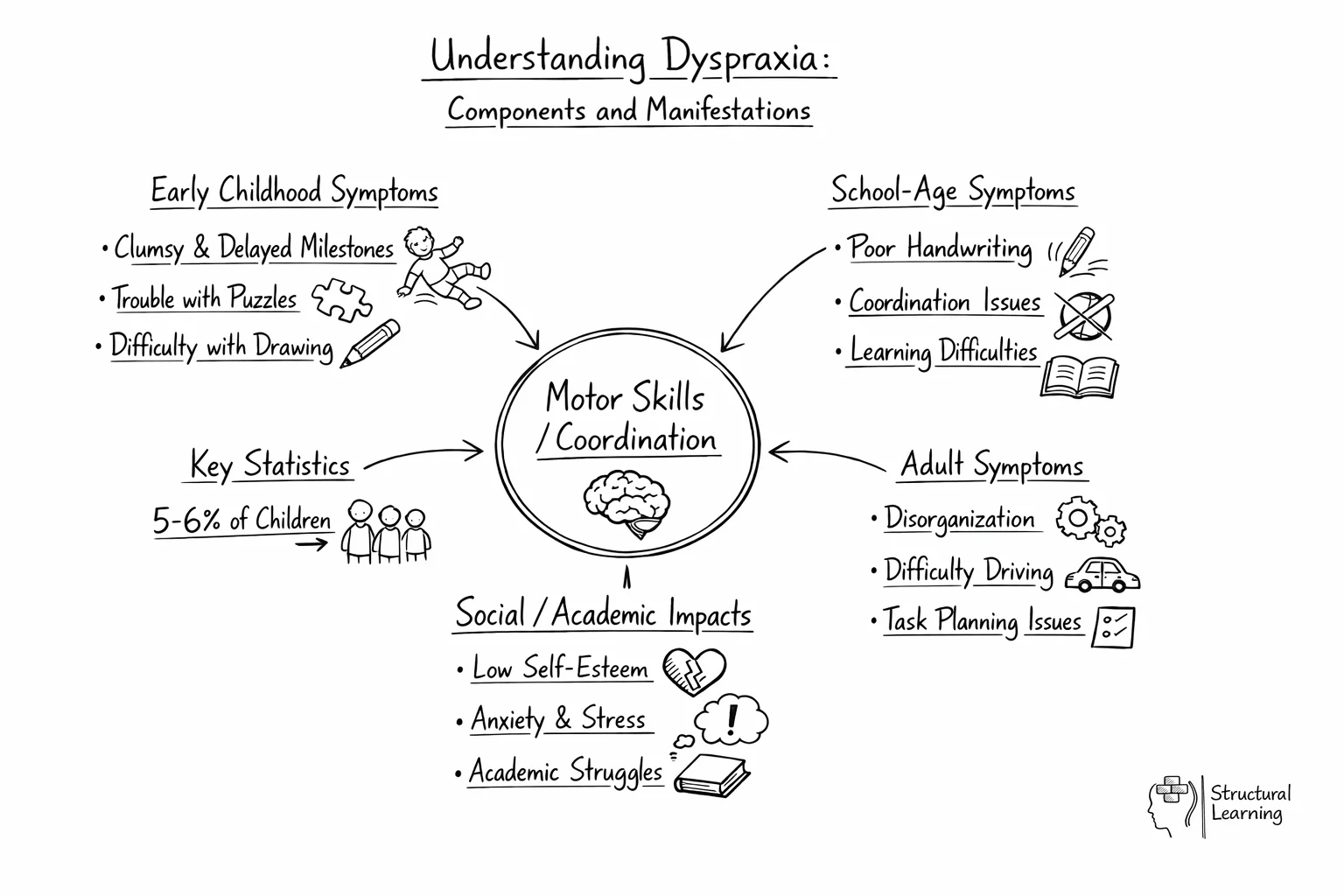
In early years, dyspraxia may show as delayed motor milestones. Learners may walk later than peers, avoid climbing frames, find scissors and pencils hard to control, or struggle with buttons, zips and shoelaces. Some avoid construction toys and jigsaws because the motor planning demand is too high. Verbal dyspraxia affects the planning and sequencing of speech movements (Kirby, 2011; Dewey et al., 2007).
Fine motor skills impact early learning. A teacher may see a learner avoid climbing. The learner may grip a pencil with their fist, unlike peers. They may struggle to catch a ball or become upset changing for PE.
By KS1, the gap between a dyspraxic child and their peers becomes more visible. Handwriting is often the most obvious difficulty: letters are poorly formed, inconsistently sized, and produced slowly with visible effort. The child may press too hard or too lightly on the paper. Sitting still at a desk is exhausting because maintaining posture requires the same motor planning that other children do without thinking.
Learners may struggle to ride a bike or scooter. They may have problems with PE, like hopping or balancing. Messy eating and losing belongings is common.
Poor task planning affects motor skills development (Kirby & Drew, 2003). This can affect learners' participation (Cairney et al., 2005).
In KS2, academic demands increase and dyspraxia creates wider consequences. The child may avoid writing tasks entirely, not because they lack ideas but because the physical act of writing is so demanding that they cannot think and write simultaneously. This is a cognitive load problem: the motor task of forming letters consumes working memory that should be available for composing sentences.
Learners may show social issues. Breaktime games become awkward. Group tasks like science, art, or DT are stressful.
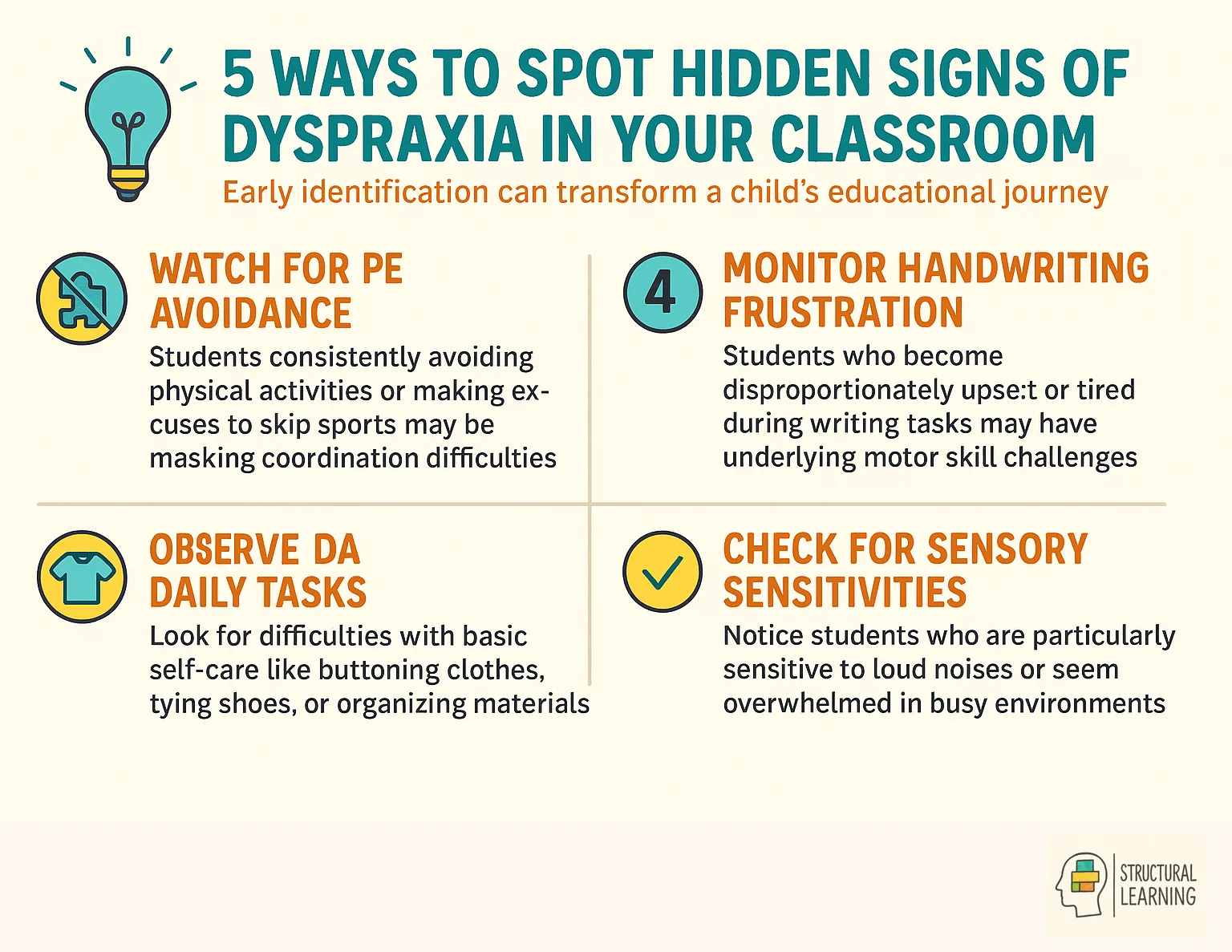
Learners may avoid PE, "forget" kit, or claim illness because public motor failure can be socially exposing. DCD is associated with higher internalising symptoms, including anxiety and low mood, so teachers should treat repeated PE avoidance, isolation in playground games and reluctance in group practical work as wellbeing evidence, not poor attitude (Omer et al., 2019; Blank et al., 2019).
Learners in Key Stage 2 often struggle with organisation. They may have trouble with homework (Alloway & Gathercole, 2006). Managing timetables and packing bags can prove hard.
Moving between classes can also be difficult. This involves motor planning, which means planning and carrying out movements. Dyspraxic learners find these tasks very challenging (Kirby & Drew, 2003).
Teachers can mistake DCD, dyslexia and dyscalculia for each other. All three can lead to low marks, frustration and avoidance. Accurate identification matters because each learner needs a different classroom adjustment.
A learner with DCD may need less handwriting and adapted equipment. A learner with dyslexia may need structured reading support. A learner with dyscalculia may need number-sense teaching (Blank et al., 2019). Start with the task barrier, not the label.
The overlap between conditions is important. Kaplan et al. (1998) remains useful historically, but schools should not rely on one older percentage. Current neurodevelopmental thinking treats DCD, ADHD, dyslexia and language needs as profiles that often overlap, so learners need broad screening, not one-condition referral routes (Gillberg, 2010; Blank et al., 2019). This means a learner referred for one condition should also be screened for others, as a child who appears to have "just" handwriting difficulties may have underlying motor coordination problems (DCD), phonological processing difficulties (dyslexia), or both.
No single test can diagnose dyspraxia. Identification should draw on several types of evidence. These include developmental history, parent and teacher evidence, standardised motor assessment, impact on daily functioning and consideration of other explanations (NHS, 2023; Blank et al., 2019; SASC, 2025).
Step 1: Teacher and parent concerns. Most referrals start when a teacher or parent notices ongoing motor coordination difficulties. The school should record clear observations as part of graduated SEN Support evidence.
This includes which tasks the learner struggles with, how their performance compares to peers, what strategies have been tried, and whether the difficulties are consistent across settings (Department for Education and Department of Health, 2015). This evidence forms the basis of a referral.
GPs can refer learners to paediatricians or occupational therapy (OT). Schools also refer learners to OT in many areas. The SENCO manages school referrals, providing teacher evidence. (Step 2; adapted from Case-Smith & O'Brien, 2015; Law et al., 2021; Missiuna et al., 2015).
Occupational therapists use structured tools to assess motor skills and daily functioning. Current assessment may include the Movement Assessment Battery for Children, Third Edition (Movement ABC-3), Movement ABC-2 where still used locally, BOT-2, Beery VMI and DASH handwriting measures. Schools may also use screening evidence from the Movement ABC-3 Checklist, which records everyday gross and fine motor coordination, and parent questionnaires such as the DCDQ for children aged 5 to 15 (Pearson, 2025; Wilson et al., 2009). These tools guide referral and support planning, but they do not replace professional diagnosis.
DCD diagnosis follows the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. A learner's motor coordination must be below the level expected for their age. It must affect daily life or schoolwork, start early in development and not be better explained by another medical, neurological or intellectual condition (American Psychiatric Association, 2022).
After assessment, the occupational therapy report should give clear recommendations for home and school. These may include classroom changes, intervention programmes, access arrangements and strategies for parents or teachers. School leaders should also keep pre-diagnostic evidence, such as records of needs-led support, reviewed adjustments and impact data. This evidence can support SEN Support decisions and EHCP discussions without forcing families into private assessment costs (Department for Education and Department of Health, 2015).
Research by Smythe and Stirling (2003) and Kirby (2011) shows simple support works best. Teachers can help dyspraxic learners with small classroom changes. These adjustments often assist other learners too, say Nicolson and Fawcett (2007).
Handwriting and written output. Reduce the physical demand of writing wherever possible. Allow the learner to use a laptop or tablet for extended writing tasks. Provide lined paper with wider spacing, and consider a writing slope (a slanted board) that improves wrist position and reduces fatigue.
Teach keyboard skills directly. By secondary school, typing becomes the main way to write for most dyspraxic learners. When you assess content knowledge, do not mark them down for poor presentation.
Dyspraxic learners may find organisation tricky, because sequencing uses motor skills (Kirby, 1999). Put a visual timetable on their desk. Give learners clear instructions, one step at a time.
Allow extra time to move between tasks (Portwood, 2000). A desk buddy helps them quietly recall needed items.
PE and physical activity. Never exclude a dyspraxic learner from PE. Instead, adapt activities so they can take part in a meaningful way.
Replace competitive team sports with individual challenges: "Can you improve your own time?" rather than "Which team wins?" Break complex movements into smaller steps and allow extra practice time. Use targets that are closer and larger. Celebrate effort and personal improvement rather than comparison with peers.
Fine motor activities. In art, design technology, and science, provide alternatives to tasks requiring precise fine motor control. Allow the use of larger tools (thicker paintbrushes, larger scissors with spring-return handles).
Pre-cut materials when the cutting itself is not the learning objective. Pair the learner with a partner who can handle the physical manipulation while the dyspraxic learner contributes ideas and planning.
Dyspraxic learners notice when tasks are hard for them (Kirby, 1999). This can cause frustration and anxiety. Celebrate each learner's strengths to build their confidence.
Many dyspraxic learners are creative and good at problem-solving. Provide chances to show off these skills publicly. A growth mindset, valuing effort (Dweck, 2006), really helps all learners.
If a dyspraxic learner has occupational therapy support, ask the therapist for exercises you can use in class. Many OT programmes include short "motor breaks" (alertness and coordination activities). Hand-strengthening exercises also take only a few minutes each day. Build them into daily routines, rather than relying only on weekly sessions.
Dyspraxia is not curable, but it is highly manageable with the right interventions. The goal is to help the child develop compensatory strategies and build the motor skills they can improve, while reducing the impact of difficulties that will persist.
Teachers should consider referral when motor barriers continue after classroom support. For post-pandemic KS1 and KS2 cohorts, compare a child's performance with their teaching history, attendance, outdoor play and chances to practise. Lockdown research is mixed rather than a simple story of universal motor delay: den Uil et al. found no overall negative effect in one Dutch cohort, but also warned that local context and individual differences matter (den Uil et al., 2023). Do not diagnose a learner from a single weak ball-catching, scissor or handwriting score if they have had limited opportunity to practise the task (SASC, 2025).
Early motor support helps, but referral should not be the first support a learner receives. Start with low-cost classroom adjustments, record what changes, and escalate when difficulties persist across settings. This gives specialists better evidence and gives the learner support while waiting lists move.
Early identification helps teachers act before learners avoid tasks or lose confidence. Teachers should record the signs clearly. This helps occupational therapists, SENCOs and families decide the next step. Early support also helps learners manage physical coordination barriers while assessment is arranged (Sugden & Wright, 1998).
Current studies indicate that developmental coordination disorder affects approximately five to six per cent of school-age children (Blank et al., 2019). This statistic suggests that most classrooms will contain at least one or two learners who require specific support for their motor skills. While boys are more frequently referred for assessment, evidence suggests that many girls are missed because their symptoms are less visible.
Teachers often wrongly assume learners lack motivation when they don't produce work. Writing tires learners, leaving less energy for lesson content. Complex instructions confuse learners who struggle to sequence steps while moving.
For handwriting, teachers should focus on the quality of the content rather than the neatness of the letters. Providing alternative ways to record information, such as voice recorders or printed diagrams, can help the learner demonstrate their true knowledge. Teachers should encourage learners to practise their motor skills in short, frequent bursts to build confidence without causing physical exhaustion.
Dyspraxia tests help schools describe motor barriers, but they do not explain every learning difficulty. A low Movement ABC score is not a full diagnosis on its own. DCD identification should include standardised motor testing, developmental history, daily functioning, chance to learn the task and exclusion of other explanations (Blank et al., 2019; SASC, 2025). In class, poor handwriting may reflect motor coordination, ADHD-related inattention, anxiety, visual tracking, weak teaching in letter formation or limited practice.
This is why executive function matters. Gillberg's ESSENCE framework shows that early motor problems often overlap with ADHD, autism, language difficulties, dyslexia and emotional needs (Gillberg, 2010). DCD research also points to cognitive-motor integration differences. This means differences in how thinking and movement work together, not simple clumsiness, so screening should ask what breaks down during the task: balance, sequencing, working memory, inhibition, planning, fatigue or social pressure (Subara-Zukic et al., 2022).
Standardised tasks can also carry cultural and socioeconomic bias. A learner with little access to bikes, balls, scissors, outdoor space, swimming, clubs or adult coaching may perform poorly because of opportunity, not DCD. This matters for working-class learners, recent arrivals and some EAL learners whose early motor experiences may not match the assessment's assumed tasks. SASC guidance therefore stresses age and opportunity to learn motor skills, not age alone (SASC, 2025).
The main practical barrier is access. NHS referral routes, occupational therapy thresholds and private assessment costs can delay identification, especially for lower-income families.
Schools should not wait for a formal diagnosis before giving support. A needs-led approach means making reasonable adjustments, recording impact, reviewing the SEN Support plan and using that evidence for EHCP discussions when needs remain significant. Careful assessment still has value, but only when it leads to quick changes in teaching rather than another year of waiting.
Ball (2024).
| Feature | Dyspraxia (DCD) | Dyslexia | Dyscalculia |
|---|---|---|---|
| Primary difficulty | Motor coordination and planning | Phonological processing and word decoding | Number sense and mathematical reasoning |
| Affects handwriting | Yes: poor letter formation, inconsistent sizing, slow speed | Sometimes: letter reversals, spelling errors | Rarely: only when writing numbers |
| Affects reading | Indirectly: tracking text across the page can be difficult | Yes: decoding, fluency, and comprehension | No, unless the text contains numerical information |
| Affects PE and sport | Yes: catching, throwing, balancing, team sports | No | No |
| Affects daily living | Yes: dressing, eating, personal care, organisation | Mainly time management and written communication | Money handling, time-telling, measurement |
| Prevalence | 5 to 6% of children | 10 to 15% of the population | 3 to 6% of the population |
| Diagnosed by | Occupational therapist, physiotherapist, or paediatrician | Educational psychologist or specialist teacher | Educational psychologist or qualified Specialist Teacher/Assessor with a current Assessment Practising Certificate for dyscalculia assessment (British Dyslexia Association, 2026) |
| Co-occurrence | Often overlaps with dyslexia, ADHD and other neurodevelopmental needs | Frequently co-occurs with DCD, ADHD | Often co-occurs with dyslexia and ADHD |
Barnett et al. (2020).
Blank et al. (2019).
Cairney et al. (2005).
Cousins (2015).
Dweck (2006).
Gillberg (2010).
Green et al. (2005).
Kaplan et al. (1998).
Kirby (2007).
Kirby (2011).
Kirby (1999).
Kirby et al. (2011).
Kirby et al. (2008).
Missiuna et al. (2006).
Peters et al. (2009).
Polatajko and Mandich (2004).
Portwood (2000).
Reynolds (1981).
Rodger et al. (2021).
Rose (2023).
SASC (2025).
Stein (2004).
Subara-Zukic et al. (2022).
Sumner (2021).
Zwicker et al. (2018).
These studies give teachers evidence to support learners.
DCD in Children: A Practical Guide for Primary School Teachers View resource ↗
National Association for Special Educational Needs (Nasen).
Nasen's guide helps teachers use research. It covers spotting needs, referral routes and classroom changes for primaries. Checklists and templates are included for immediate use (Nasen, n.d.).
The Dyspraxia Foundation: Information for Teachers
Dyspraxia Foundation UK.
Researchers like Kirby et al. (2011) and Sugden (2007) provide valuable insights. The Dyspraxia Foundation offers resources for UK teachers.
These resources include classroom strategy sheets and referral process details. Use the pack to explain dyspraxia to learners and parents. The free pack is updated with current research findings.