Conners Rating Scale: How to Score, Interpret, and Use It in School
Conners rating scale guide beyond the basics. Score each version, interpret T-scores, and translate results into practical classroom support.


Conners rating scale guide beyond the basics. Score each version, interpret T-scores, and translate results into practical classroom support.
What is the Conners rating scale?
The Conners rating scale is a standardised questionnaire used to record ADHD-related behaviours across home and school settings. It supports assessment but does not diagnose ADHD on its own—NICE guidance is clear that diagnosis needs a full clinical picture. For teachers, it offers a structured, comparable way to describe a learner's behaviour.
Conners Rating Scale: How to Score, Interpret, and Use It in School describes a standardised behaviour rating tool used to record ADHD-related behaviours across home and school. It does not diagnose ADHD by itself. NICE guidance says rating scales such as Conners can support assessment, but diagnosis needs clinical judgement, developmental history, observer reports, and evidence across settings (NICE, 2018).
For example, if a Year 6 learner leaves the carpet six times during a 15-minute input, loses equipment daily, and needs repeated prompts to start writing, the Conners form helps the teacher report those patterns clearly. The score matters, but the written examples often matter more because they show when the behaviour happens and what else could explain it.
Dr Keith Conners created the Conners Rating Scale in 1969. It helped clinicians assess treatments on learner behaviour. The Conners 4, released by MHS, is the newest version. It is more precise and represents diverse groups better.
Conners (undated) compares a learner's behaviour with peers and notes inattention. SENCOs can use it for assessment purposes. Conners 4 (undated) showed that Leo's disorganisation reflected weak executive function. This moved the focus to Leo's neurology, not attitude.
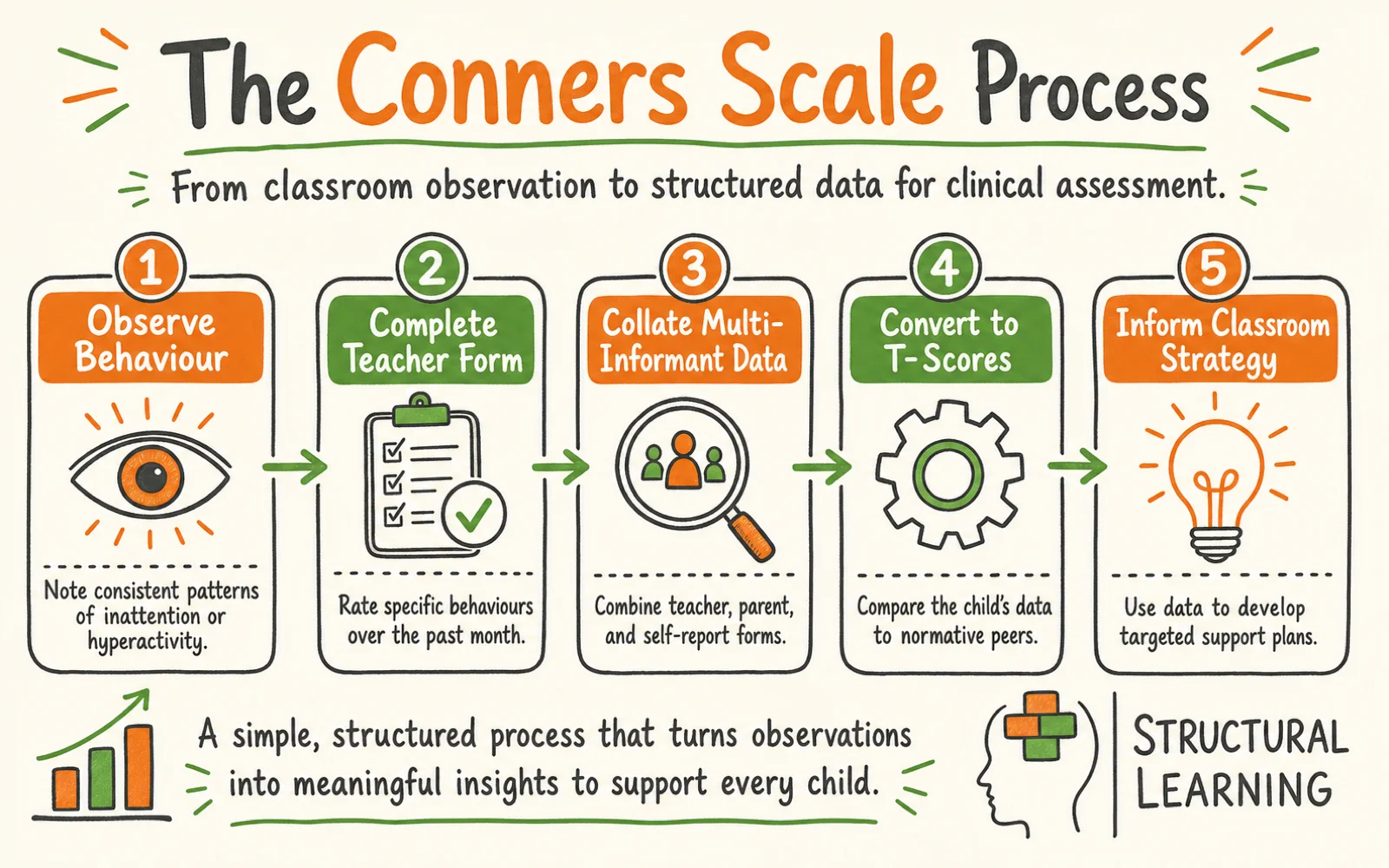
The strength of the Conners system lies in its 'multi-informant' design. ADHD is a pervasive condition, meaning it should show up in more than one area of a child's life.
To get a full picture, the assessment usually involves three different forms. There is a parent form, a teacher form, and, for children aged eight or older, a self-report form. Each person sees a different side of the child.
Teachers see attention, organisation, movement, and peer interaction under real classroom demand. A learner may cope at home because the setting is quieter and adults can adjust quickly.
In a Year 9 science lab, the same learner may struggle with instructions, equipment, noise, and peer pressure at the same time. The clinician needs this contrast between home and school, because ADHD assessment depends on patterns across settings, not one person's view.
At a secondary school in Manchester, a learner named Sarah was struggling. Her parents said she was helpful and quiet at home, while her teachers' Conners 4 forms showed high inattention scores.
Sarah was not challenging lessons. She was absent during explanations, especially when cognitive load increased. Without the teacher form, the GP may have missed how strongly her difficulties appeared in school, which is common in the inattentive presentation of ADHD in girls.
The Conners 4 Teacher Form is designed to be completed quickly but requires careful thought. It consists of a series of statements about the child's behaviour over the past month. On the Conners 4, each statement is rated on a 4-point scale: 0 = 'Not true at all (Never/Rarely)', 1 = 'Just a little true (Occasionally)', 2 = 'Pretty much true (Often/Quite a bit)', and 3 = 'Completely true (Very often/Always)' (Conners 4 Manual, MHS). The 'Not true at all (Never, Seldom)' ... 'Very much true (Very often, Frequently)' wording belongs to the older Conners 3.
The questions cover several distinct 'content scales'. These include:
You will see statements like "Does not seem to listen when spoken to directly" or "Leaves seat in situations when remaining seated is expected." It is important to answer these based on what you have actually seen, not what you think the child is capable of if they 'just tried harder'.
Take Mr Thompson, a Year 6 teacher. He was filling out a form for a learner named Ben. He noticed several questions about 'Impulsivity'. He remembered that Ben often jumped into the middle of games at break time without asking and blurted out answers before Mr Thompson had finished the question.
By marking these as '3, Very much true', he provided the clinician with evidence that Ben struggled with inhibitory control, which is a core feature of ADHD.
Once you return the form to the SENCO, the raw scores are calculated and converted into 'T-scores'. This is where the clinical magic happens.
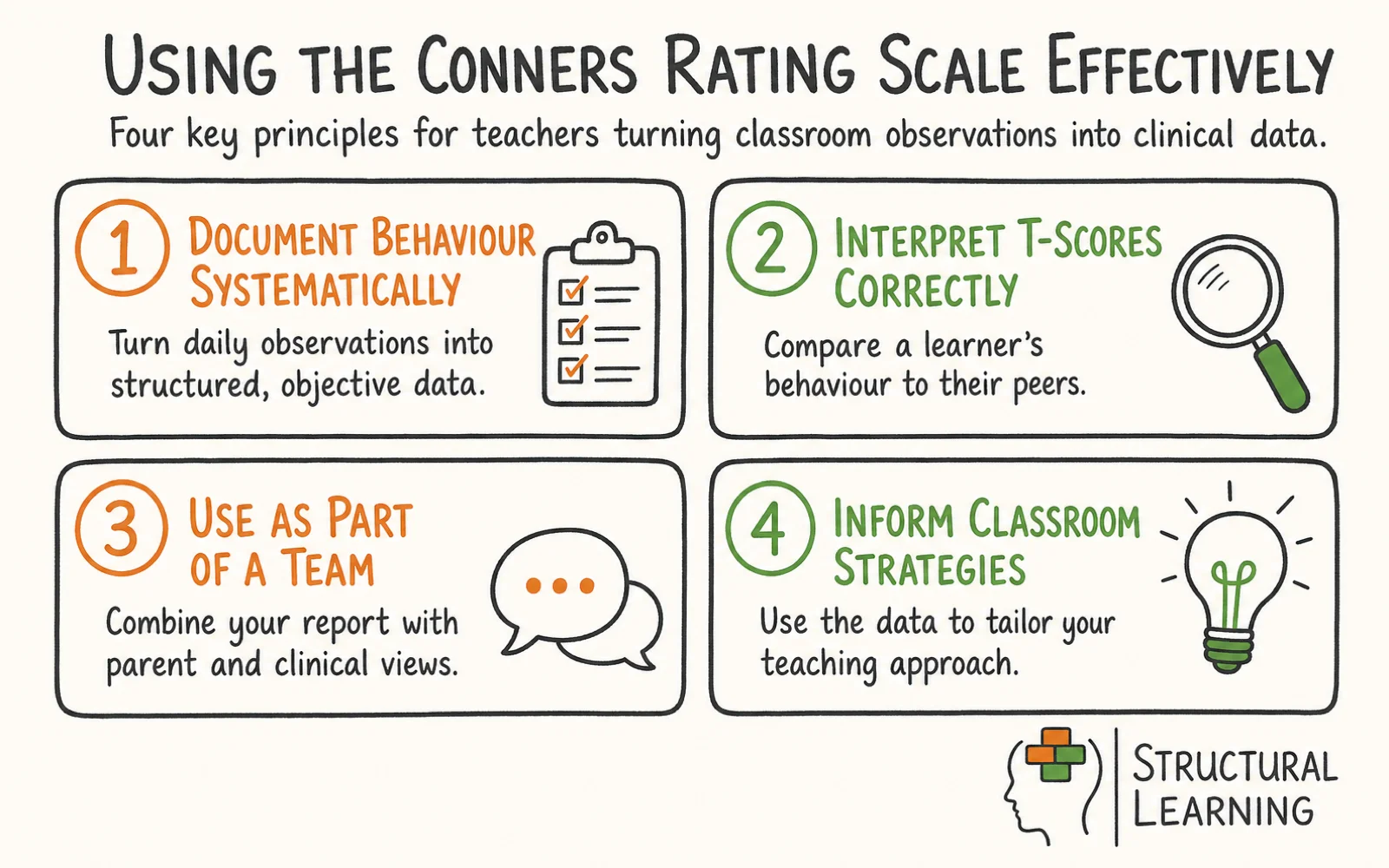
A T-score is a way of comparing that specific child to a huge database of children of the same age and gender. The mean (average) T-score is 50. The scale uses standard deviations of 10 to show how far a child is from the norm.
Here is the general breakdown used by UK professionals:
When a SENCO looks at a report, they aren't just looking for one high number. They are looking for a profile. A child might have a T-score of 45 for hyperactivity but a 75 for inattention. This tells us they have the inattentive presentation of ADHD.
In a staff briefing at a school in Birmingham, the SENCO explained a report for a Year 2 girl named Amara. Her 'Inattention' T-score was 72, but her 'Hyperactivity' was only 48. The class teacher had been worried because Amara was so quiet, but the T-scores showed that her internal distraction was as severe as a child who was physically running around the room. This helped the teacher understand that Amara needed visual prompts and 'check-ins' rather than behavioural management.
The final report usually includes a visual profile or a bar chart showing these T-scores. As a teacher or SENCO, you need to look at the patterns.
The most interesting part is often the comparison between the teacher and parent scores. Sometimes they match perfectly, which gives a very clear picture of the child's needs. Other times, they are very different.

If a teacher reports high scores and a parent reports typical scores, it does not mean someone is wrong. It may show that the school setting places heavier demands on attention, organisation, waiting, and peer regulation.
This is where the Conners can reveal classroom friction as well as learner need. Timimi (2018) warns that ADHD ratings can reflect social tolerance for behaviour as much as underlying impairment. SENCOs should therefore read scores alongside lesson structure, teacher workload, class size, trauma history, sleep, anxiety, and family context.
For example, a SENCO at a secondary academy reviewed the Conners for a Year 10 learner. Parents marked 'Emotional Dysregulation' as very high. Teachers marked it as typical.
In the meeting, staff realised the learner was suppressing anxiety all day because he feared getting things wrong. His frustration then came out at home. The school gave him a quiet space at lunchtime so he could regulate before the end of the day.
High Conners scores do not mean a learner has ADHD. Only UK clinicians diagnose ADHD, usually paediatricians or psychiatrists. The Conners test offers one piece of evidence. Clinicians also review the learner's history and school reports, maybe observing them (NICE, 2018).
Once the Conners scores are in, the SENCO usually decides what to do next. High scores may support a referral to CAMHS (Child and Adolescent Mental Health Services). They may also support a referral to a local paediatric neurodevelopmental pathway or an Educational Psychologist assessment.
For headteachers, this is also a resource decision. The Conners can become a bottleneck for SEND evidence, EHCP paperwork, exam access arrangements, and specialist referral. Treat it as a clinical support tool and an operational record, not as a form to complete in isolation.
At a primary school in Norfolk, Conners 4 results for a Year 4 learner led to an immediate School Support Plan. Before the CAMHS appointment arrived, the school used the Executive Function score to justify a personal workstation and a visual timetable.
The team did not wait for a diagnosis before acting. The same evidence later supported an EHCP (Education, Health and Care Plan) application because it showed need, provision, and impact over time.
The Conners isn't the only tool in the box. You might hear people talking about the Vanderbilt, the SNAP-IV, or the SDQ. It is helpful to know the difference so you can understand why your SENCO has chosen a specific form.
The SNAP-IV-26, a free alternative to the Conners, has 26 items drawn from DSM-IV criteria: 18 ADHD symptom items plus 8 oppositional defiant disorder items (Bussing et al., 2008; SNAP-IV-26 scoring guide). The 18 ADHD symptom descriptions carried over essentially unchanged into DSM-5, but the scale itself is DSM-IV-based. Teachers complete it in 10 minutes. Schools often use SNAP-IV to screen learners before Conners assessment.
The SDQ (Goodman, 1997) screens for emotional, conduct, hyperactivity, and peer issues. However, the SDQ lacks specific ADHD details.
The Vanderbilt (VADRS) is often used because it is free and covers the DSM-5 criteria for ADHD. It is a useful screening tool, but it does not have the depth of the Conners 4. The SNAP-IV is another quick rating scale often used in clinical settings to monitor whether medication is working.
The SDQ (Strengths and Difficulties Questionnaire) is common in UK schools, but it is a general mental health screen. It covers anxiety, conduct, peer problems, and hyperactivity. The BRIEF-2 is narrower: it focuses on executive function, or how the brain manages tasks.
Conners 4 subscales align with DSM-5-TR criteria (APA, 2022). The DSM-5-TR describes three ADHD types: Inattentive, Hyperactive/Impulsive, and Combined. Each needs 6+ symptoms.
T-scores above 65 suggest more symptoms; 70+ shows clinically significant levels. SENCOs understanding this can use targeted support for each learner. See our ADHD guide for assessment.
A SENCO in a Kent secondary school recently decided to use the BRIEF-2 alongside the Conners 4 for a learner who was failing every subject. While the Conners showed high inattention, the BRIEF-2 showed that the real issue was ''Working Memory' and 'Task Initiation'. This meant that instead of just telling the learner to 'pay attention', the teachers started giving him task checklists and breaking long assignments into five minute chunks. The Conners identified the problem, but the BRIEF-2 helped refine the solution.
When you sit down with a Conners form, your mindset matters. It is easy to fill it out after a particularly difficult Friday afternoon when your patience is thin. However, the clinician needs an objective view of the child's 'typical' behaviour over the last month. Here are some ways to ensure your input is as accurate as possible.
First, observe the learner in different contexts. ADHD-related behaviours can look different during silent reading, a transition, a practical lesson, and a noisy PE session. Second, be specific. Replace "He's always annoying" with a count, time, place, and trigger.
Third, check culture, language, trauma, sleep, bereavement, hearing, and recent family change. Gillborn (2008) shows how school systems can misread behaviour through racialised expectations. For items about defiance or authority, give clear examples. This helps stop cultural misunderstanding becoming a high T-score.
A Year 1 teacher in London had a learner who was very restless. Instead of completing the form straight away, she kept a three-day tally of how often the learner left his seat during carpet time.
When she completed the Conners, she could mark '3, Very much true' for the hyperactivity questions and add the count as evidence. This made her report stronger when the SENCO met the parents.
The main misconception is that a high Conners score means a learner has ADHD. It does not. The scale records behaviours, not causes. Use it as a starting point for professional discussion: identify the learner's current need, record evidence from more than one lesson, and agree the next classroom adjustment with the SENCO or family.
Anxiety, trauma, sleep loss, hearing difficulty, family stress, or grief can all look like inattention or restlessness. This risk is higher after the pandemic, because ADHD symptoms increased across many child samples during COVID-19 disruption (Rogers and MacLean, 2023), and national behaviour data now show changed school behaviour patterns in England (DfE, 2025). Use current observation notes, not the T-score alone.
Another misconception is that the scale is biased against boys. While it is true that boys are diagnosed more frequently, the Conners 4 has been designed to look for the 'internalised' symptoms often seen in girls. Finally, some people think that completing the Conners is a step towards 'drugging' children. In the UK, medication is only ever one part of a multi modal treatment plan, and the decision is made by doctors and parents, not by the school or the rating scale.
A Year 8 tutor once spoke with a parent who feared the Conners would become a label for life. The tutor explained that the form could help the school document exam access needs.
By showing severe functional impairment, the school could make a stronger case for 25% extra time where the learner met the access arrangements criteria. The point was not to label him. It was to record the barrier clearly enough for support to follow.
How long does it take to complete?
The teacher form usually takes about 15 to 20 minutes. It is best to do it in one sitting in a quiet place so you can focus on the child.
Can I refuse to complete it?
Technically, yes, but it is considered part of your professional duty to support the SEND process. If you feel you don't know the child well enough (for example, if you have only taught them for a week), you should tell your SENCO.
Who sees the results?
The scores are shared with the SENCO, the parents, and the medical professionals involved. They are kept as part of the child's confidential SEND file.
Do I need special training?
No. You just need to follow the instructions on the form. The interpretation is done by the SENCO or the clinician using a scoring manual.
How often is the assessment repeated?
It is often done once at the start of the assessment process. If a child starts medication or a new intervention, it might be repeated six months later to see if the scores have improved.
What if I disagree with the results?
The report is a snapshot of one point in time. If the results don't match your experience, speak to your SENCO. It might be that the child is presenting differently in your specific subject or that something has changed in their life since the form was completed.
Your next step is to speak with your SENCO about any child in your class whose behaviour is consistently out of sync with their peers. Ask if a Conners 4 screening would be appropriate to help identify their specific support needs (Conners, 2008).
Differentiation is important. Research on inclusive pedagogy suggests structured differentiation reduces barriers for learners with additional needs (Florian & Black-Hawkins, 2011).
Rose & Meyer (2002) show UDL can help. Use our free differentiation resource pack for learners and staff. It includes posters, desk cards, and CPD materials.
Conners-3 (2008) checks learner inattention and builds upon earlier tests. Validity scales show if learners answer inconsistently. When first published, the Conners 3 teacher form's DSM Symptom Scales aligned with DSM-IV-TR criteria (Conners, 2008); MHS released a DSM-5 Update in January 2014, so current Conners 3 scoring aligns with DSM-5, and the successor Conners 4 (MHS, 2022) uses current DSM criteria (source: MHS Conners 3 DSM-5 Update document; MHS Conners 4 manual).
The Conners-3 has shorter forms, easing teacher workload (Conners, 2008). These help when assessing many learners at once. A Conners-3 teacher report does not mean a full 115-item form was used. Knowing the version helps teachers understand the report's scope (Conners, 2008).
Conners (2008) ratings convert to T-scores, averaging 50. T-scores over 65, near the 93rd percentile, suggest problems. Watch scores between 60 and 64; Conners (2008) sees them as possible worries.
T-scores compare learners to a typical group; they aren't a diagnosis. A high score means the learner shows more of a behaviour than their peers. Consider scores with observations and reports (Pelham, Fabiano, & Massetti, 2005). Draw conclusions about support needs using all available information.
NICE (2018) says ADHD diagnoses need proof of impairment in two settings, like home and school. Conners-3 teacher scales give quantified school impairment data, as NICE requires. Without teacher forms, clinicians lack cross-setting data for a strong diagnosis.
NICE says rating scales add to, not replace, full assessments. Teachers fill in Conners forms. This gives a fuller picture alongside interviews and history. Knowing this helps teachers value the form (Conners, 2008).
Conners-3 scales may give false positives; learners might score high without ADHD. Anxiety and trauma can worsen inattention scores (Conners, 2008). Sleep loss and family issues also affect hyperactivity scores. Bereaved learners may struggle to focus, but lack ADHD (Conners, 2008).
Qualitative feedback reduces false positives. Observation-based comments help more than ratings. Note when symptoms began, and if behaviour changed.
Check for patterns related to subjects or times (Pelham, Fabiano, & Massetti, 2005). This gives clinicians context scores miss.
The Conners Rating Scale should not be treated as a diagnosis. NICE states that ADHD diagnosis must rest on clinical assessment, developmental history, observer reports, and impairment across settings, not rating scale data alone (NICE, 2018). This matters because the scale records visible behaviour. Anxiety, trauma, sleep loss, hearing difficulty, grief, and family stress can all raise inattention or hyperactivity scores without ADHD being the cause.
Teacher ratings also carry rater bias. Abikoff et al. (1993) found that halo effects can distort ratings of ADHD and oppositional behaviour. A learner with a difficult reputation, a recent exclusion, or high movement in one lesson may receive higher scores than the same behaviour would receive from another adult. This makes written classroom examples as important as the T-score.
There are cultural and methodological limits too. Items about defiance, compliance, and peer relations can reflect school norms as well as learner need. Gillborn (2008) shows how education systems can reproduce racialised judgements. For this reason, Conners ratings must be checked against context, language, culture, and adult expectations.
Finally, norms can date quickly. Post-pandemic studies reported increased ADHD symptoms in children (Rogers and MacLean, 2023), while recent DfE behaviour surveys show changed classroom conditions in England (DfE, 2025). Even with these limits, the Conners remains valuable when schools use it as one structured evidence source, paired with observation, family knowledge, and clinical judgement.
Karpicke, J. (2008). The critical importance of retrieval for learning.
Vygotsky, L. (1978). Mind in society: The development of higher psychological processes.
Research supports Conners' Rating Scale and ADHD assessment for schools. Manuals with peer-reviewed studies give key evidence. They help teachers understand learner needs (Conners, various dates). Barkley (1997) and Brown (2006) also furthered this understanding.
Psychometric Properties of the Conners 4 Rating Scales View study ↗
3 citations
Tatar et al. (2023)
This psychometric study of the Conners 4 found acceptable reliability and confirmed the underlying factor structure across age groups. The findings reassure teachers that raised T-scores on the inattention and hyperactivity scales reflect a real pattern of behaviour rather than measurement noise.
Barkley and Murphy (1998) show many ADHD rating scale studies exist. Biederman et al. (1993) found teacher and parent reports often disagree. Miller et al. (2009) reviewed why reports vary like this. Gomez, Harvey, and Quick (1999) link agreement to better learner identification.
De Los Reyes et al. (2015)
This meta-analytic review found that informant disagreement on ADHD rating scales is the rule, not the exception, because each rater observes the child in a different context. The implication for teachers is that Conners scores from school should be triangulated with parent and clinician data rather than treated as a stand-alone signal.
ADHD Assessment in UK Schools: Current Practices and Challenges View study ↗
23 citations
Sayal, K. et al. (2018)
Teachers in the UK identify learners with ADHD symptoms, according to research. This study shows teachers are key in the assessment process. Conners scales standardise teacher input, which the authors argue improves the quality of referrals from schools to clinical assessment.
Executive Functioning Deficits in Children with ADHD: A Meta-Analysis View study ↗
82 citations
Willcutt, E.G. et al. (2005)
This meta-analysis confirmed that executive function deficits are a core feature of ADHD across attention, inhibition, and working memory. Conners 4 users should therefore weigh the Executive Functioning scale alongside inattention and hyperactivity scores when planning classroom support.
Gender Differences in ADHD Presentation: Implications for School-Based Assessment View study ↗
670+ citations
Mowlem, F. et al. (2019)
Mowlem and colleagues argue that girls with ADHD are often overlooked because their inattentive symptoms are less more visible than the hyperactive presentation more common in boys. Teachers should hold this in mind when completing Conners 4 forms, and lean on the gender-specific norms when reading the resulting T-scores.