Updated on
July 14, 2026
Childhood Trauma Tests
A guide to childhood trauma tests, the ACEs framework, screening tools like the SDQ, and trauma-informed classroom practice for teachers.


Updated on
July 14, 2026
A guide to childhood trauma tests, the ACEs framework, screening tools like the SDQ, and trauma-informed classroom practice for teachers.
Exposure to these events can be life changing; learners might have issues in later life, particularly in relation to learning. Research by Padesky (1994) and Ogden, Minton and Pain (2006) stresses the physiological impact of trauma. Van der Kolk (2014) finds that processing these experiences is key.
Research shows reactions are short-term or long-term. Short-term reactions happen right after events. Unstable emotions, flashbacks, and less contact are long-term effects. Headaches or nausea are also possible.
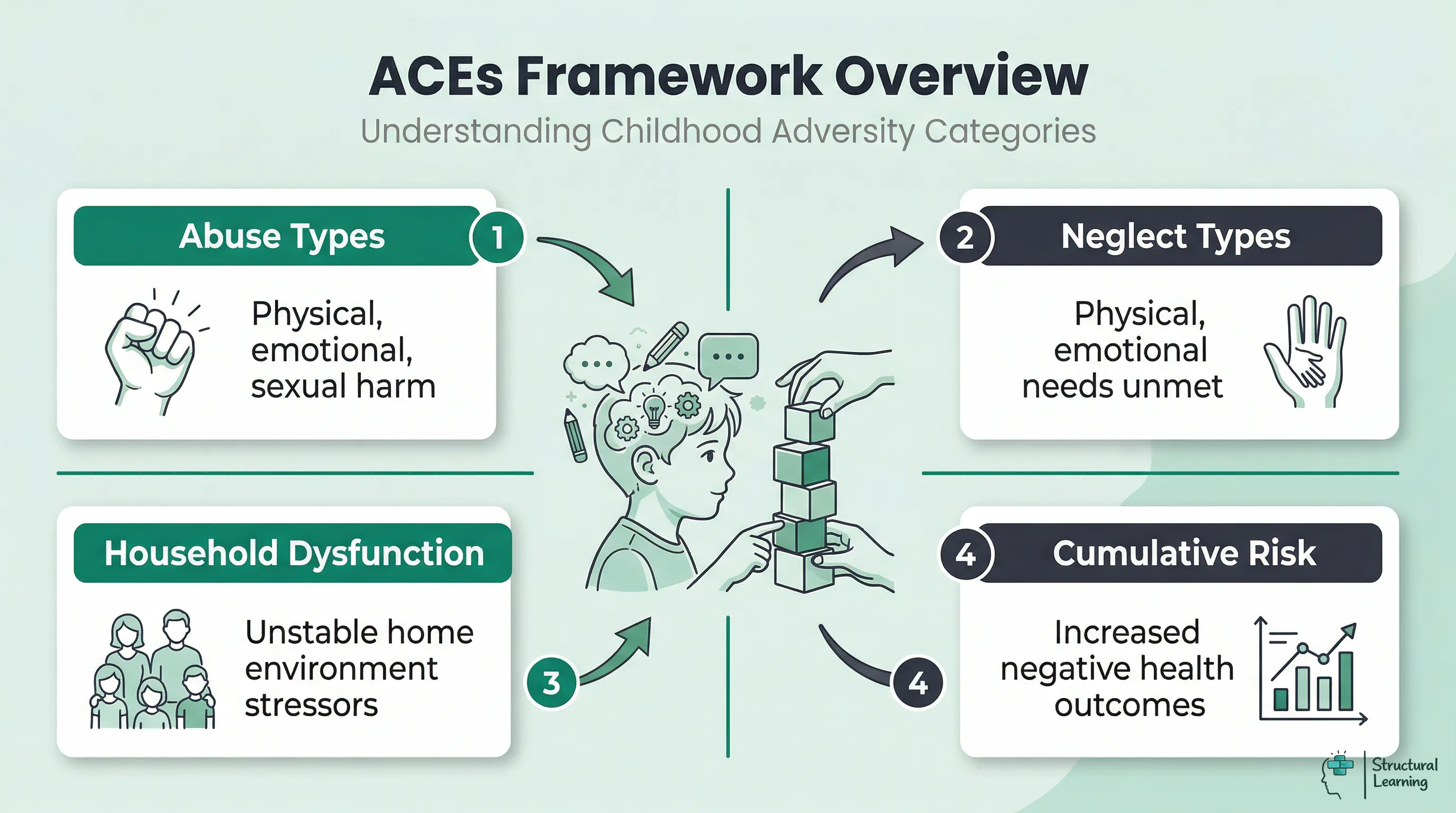
The ACEs framework, from the CDC-Kaiser Permanente study (1998), identifies ten types of childhood adversity. These ACEs measurably impact lifelong health and wellbeing. Researchers surveyed over 17,000 adults and found a link between ACEs and later problems. Experiencing more ACEs increased risk, said Felitti et al (1998).
The ten ACE categories fall into three groups:
Abuse: physical abuse, emotional abuse, and sexual abuse.
Neglect: physical neglect and emotional neglect.
These adverse experiences harm learners' wellbeing (Anda et al., 1999). Parental separation, domestic violence, or substance misuse impact learners. Mental illness or incarceration within a family also affect learners' lives (Felitti et al., 1998). These factors create challenges for learners (Hughes et al., 2017).
ACE scores rise with each adverse experience, research shows. (Felitti et al., 1998). Learners with four or more ACEs risk mental health and lower attainment. (Anda et al., 2006). Teachers should recognise disengaged learners may struggle with past trauma.
The ACE framework has limits; it misses some adversities like racism or poverty. A high ACE score doesn't guarantee negative outcomes. Protective factors, such as caring adult relationships, help learners. Teachers can be that vital protective adult (Anda et al., 1998; Felitti et al., 1998).
Although these emotions are common, some people find it difficult to go on with their life.
To further assess the potential impact of childhood trauma, a Childhood Trauma Test can be taken. This is a brief online test that evaluates an individual's potential to be affected by some type of childhood trauma. The results from this test may provide greater insight into the severity and impact of experiences in an individual's life, as well as strategies to cope with any trauma.
Learners can explore childhood experiences through writing or talking to support networks. This may help find and address trauma missed by tests. Remember, each learner's childhood is unique (Felitti et al., 1998; van der Kolk, 2014). Do not compare or judge their experiences.
If an individual feels that their trauma is more serious than what the test identified, it is recommended to seek help from a mental healthprofessional. A mental health professional is trained to address and diagnose childhood trauma. They will likely use therapeutic techniques and strategies to create a safe environment where individuals can talk about their traumas in a judgement-free space.
We will all experience both unpleasant events and joyous times. There is something inside all of us that is a result of all our memories and experiences. All of these experiences and recollections have left a mark on who we are. What do we refer to as the effect of these things? How are we affected by these events? How can we handle it? This guide will address all these queries.
Childhood trauma includes physical, emotional, and sexual abuse, plus neglect (Anda et al., 2006). Learners are also affected by domestic violence and substance abuse at home. Natural disasters, bullying, accidents, and witnessing violence all have impact (Anda et al., 2006). These traumas manifest differently in learning and emotional reactions.
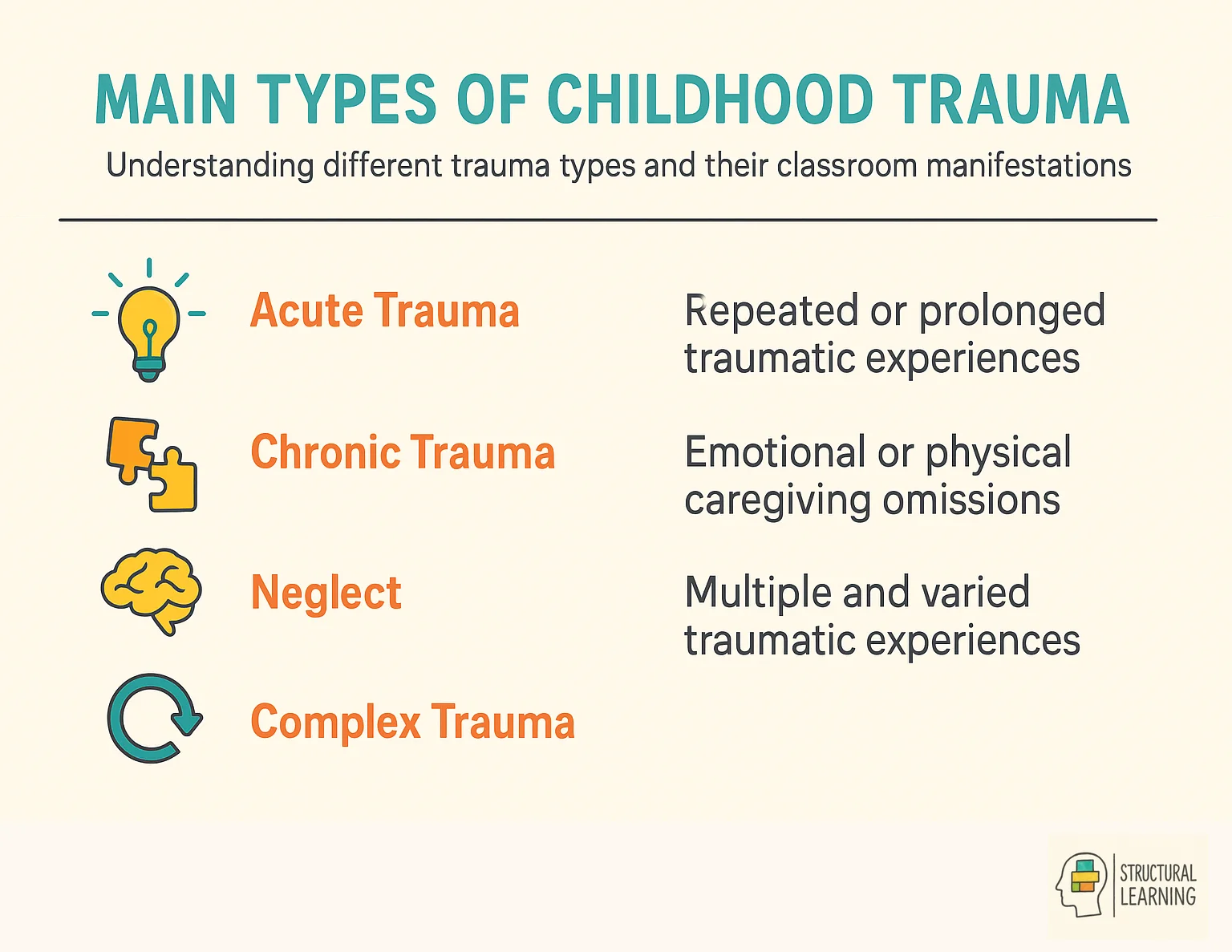
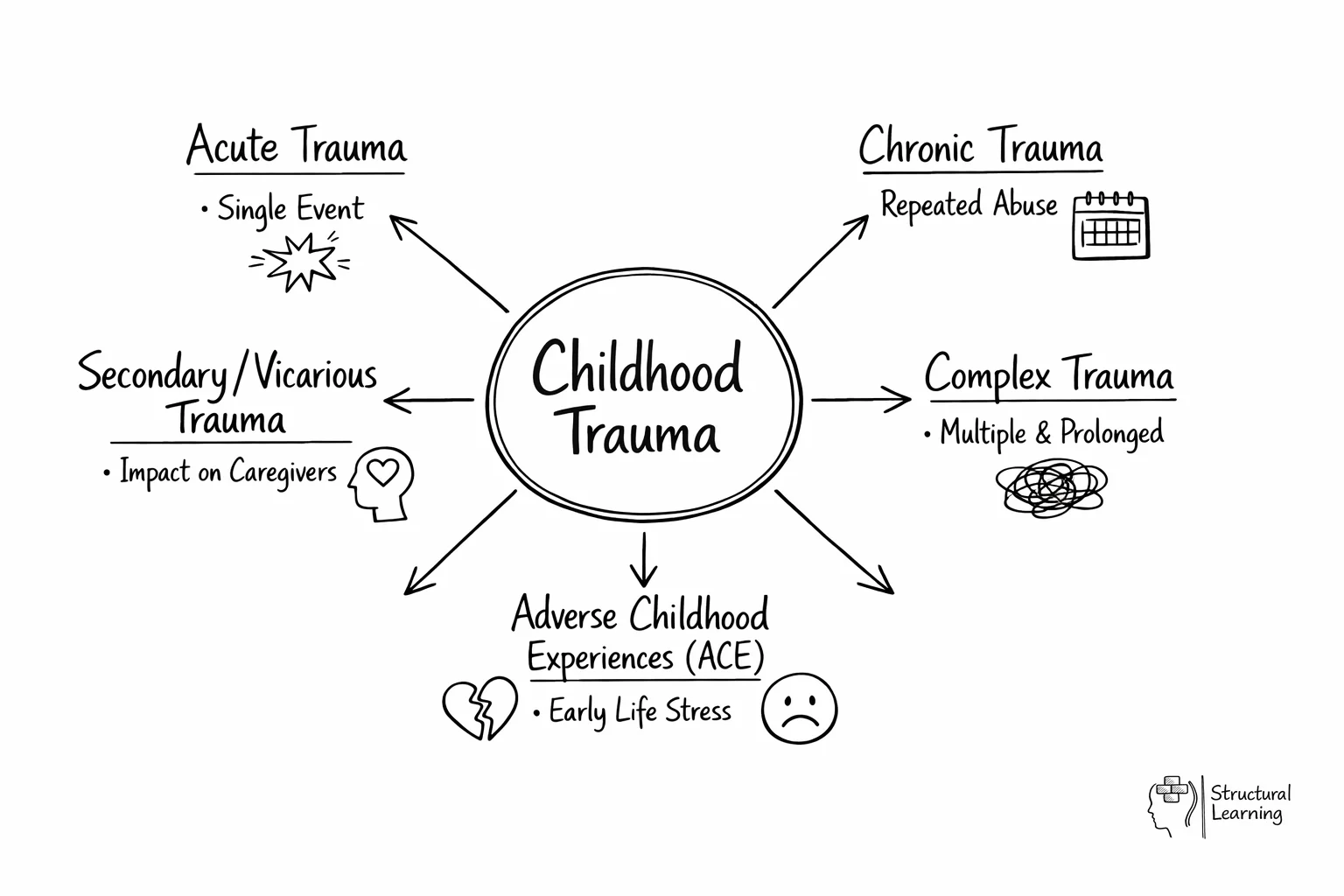
This subsection will focus on the different types of trauma and provide a short outline of each. Understanding the different types of trauma is essential since they can all have a profound impact on a person's life. It might affect a person's employment, interpersonal connections, or health.
Let's explore these types together.
Acute Trauma: represents great pain due to a single event, and the reaction lasts only briefly. A car accident, a physical or sexual attack, or the unexpected loss of a loved one are typical examples.
Chronic trauma can stem from repeated negative experiences. This may include bullying or neglect. Abuse (emotional, physical, or sexual) and partner violence are also causes (van der Kolk, 2003; Cook et al., 2005).
Complex Trauma: can occur when a person is exposed to a series of traumatic events from which they cannot recover. It includes the feeling of being tied down. Like other forms of trauma, it can impair one's sense of security in the world and lead to hypervigilance, which is the obsessive and exhausting monitoring for warning signs of danger.
Secondary trauma affects those responding to injury and disaster. (Bride, 2007) Exposure to others' pain causes this. Emotional exhaustion happens when people avoid connecting emotionally. (Figley, 1995; Stamm, 1999) This is a self-protection tactic.
ACEs are challenging experiences for developing learners (Anda et al., 1998; Felitti et al., 1998). These experiences can hinder development and cause lasting emotional harm (Anda et al., 1998; Felitti et al., 1998). Learners often lack effective coping skills when facing ACEs (Anda et al., 1998; Felitti et al., 1998).
Adverse childhood experiences include divorce, neglect, and abuse. Abuse covers emotional, physical, and sexual forms (Felitti et al., 1998). These experiences can affect a learner's well-being and attainment (Anda et al., 2006).
Childhood trauma is the key area that we'll emphasise in today's post.
You can also take an online trauma test at the link below to determine whether or not you have experienced trauma.
Https://www.clinical-partners.co.uk/for-adults/anxiety-disorders/ptsd/ptsd-test
Free learning audit
Two quick ratings and two questions. We'll show you where your school sits and send you the learner observation toolkit (PDF).
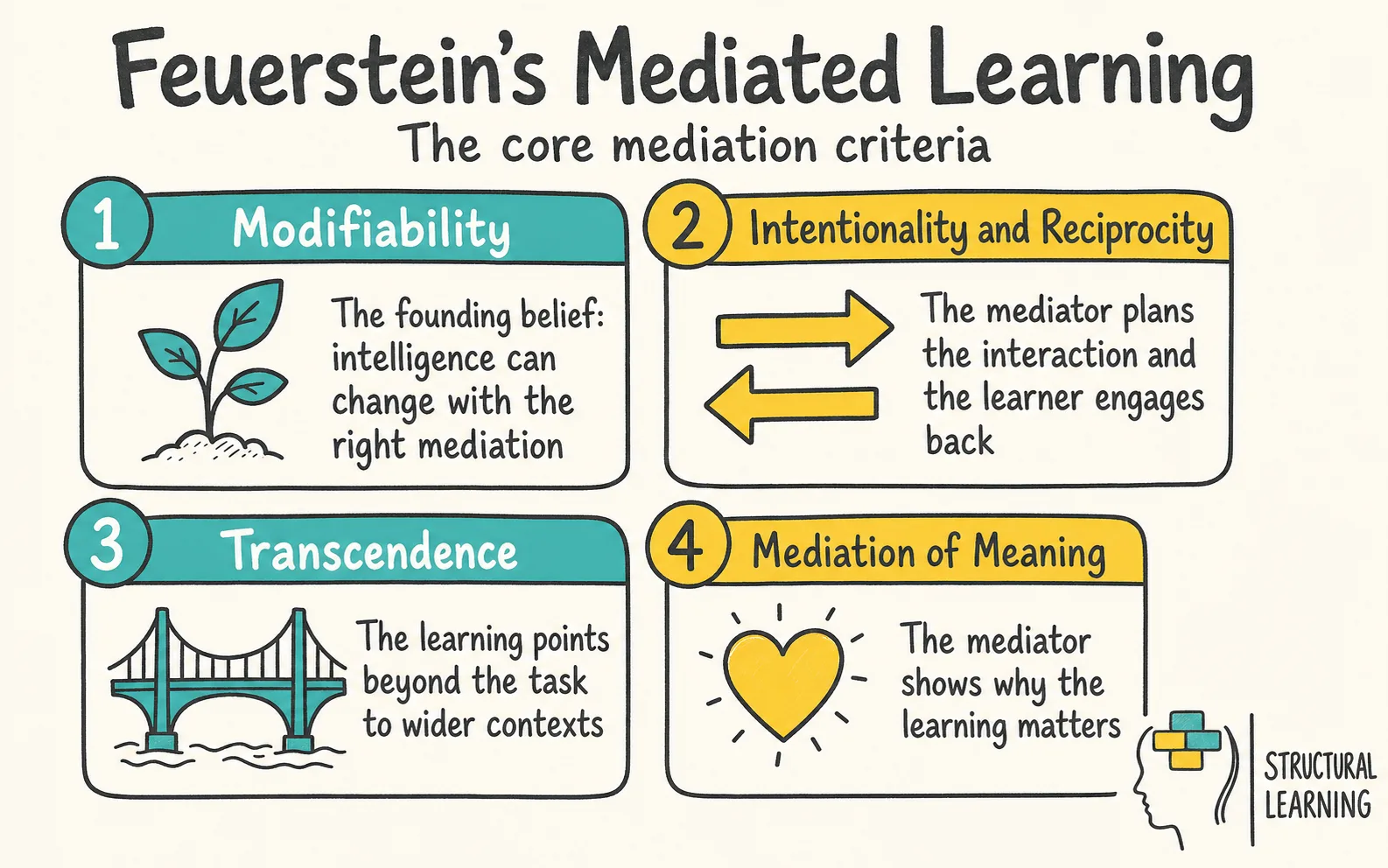
Trauma can trigger a learner's survival response from their autonomic nervous system. This system may misfire in learners with trauma, even when safe (van der Kolk, 2003). Knowing this helps teachers respond compassionately, not punitively (Bloom, 2010; Perry, 2006).
Fight: The learner may display anger, defiance, or aggression. They may argue with adults, refuse instructions, or lash out physically. This is not a deliberate choice to misbehave but an automatic protective response.
Flight: The learner may attempt to leave the classroom, hide under furniture, or mentally withdraw by daydreaming or disengaging. Running away from school or avoiding particular lessons may also indicate a flight response.
Freeze: The learner may appear to shut down completely. They may stare blankly, be unable to answer questions they normally could, or seem physically rigid. This is often misinterpreted as inattention or stubbornness.
Fawn: The learner may become excessively compliant, people-pleasing, or eager to avoid conflict at all costs. They may agree to everything, never express their own needs, and appear to have no preferences. This response is particularly easy to miss because the child does not present as challenging.
Teachers should be aware that the same child may display different responses in different situations, and that these responses can change over time. A child who was previously in freeze mode may begin to show fight responses as they start to feel safer, which can be confusing for staff who interpret this as deterioration.
Trauma impacts learners' behaviour, emotions, and thinking. Teachers must spot signs to help learners properly. Symptoms vary by age, trauma type, and coping skills (van der Kolk, 2003; Perry, 2009).
Some common signs include:
Remember learners showing these signs may have other issues. If you see many symptoms, consider trauma as a possibility. Support the learner and make referrals if needed, (van der Kolk, 2014; Perry & Szalavitz, 2006; Levine, 1997).
Teachers are not expected to diagnose trauma, but they play a critical role in identifying learners who may need further support. Several screening and assessment tools are commonly used in UK schools, each with distinct strengths and limitations.
Alongside formal screening tools, teacher observation is one of the most valuable sources of evidence. Teachers see children for six hours a day, five days a week, and are well placed to notice patterns that a one-off assessment cannot capture. When recording observations, note:
| Trauma Response | What It Looks Like in Class | What It Is Often Mistaken For | Helpful Teacher Response |
|---|---|---|---|
| Fight | Arguing, shoving, refusing tasks, verbal aggression | Defiance, poor behaviour | Lower your voice, offer space, avoid power struggles |
| Flight | Leaving seat, running from class, hiding, task avoidance | Disobedience, laziness | Agree a safe space in advance, let them return without shame |
| Freeze | Blank staring, inability to respond, physical rigidity | Inattention, stubbornness | Speak gently, give time, offer a grounding activity |
| Fawn | Over-compliance, people-pleasing, never expressing needs | Good behaviour, model learner | Actively seek their opinion, validate their preferences |
These observations are crucial evidence when referring learners to mental health or social services. Factually record what you saw and when, not learner motivation (CAMHS, social care, educational psychology).
Such classrooms reduce the impact of trauma on learners (SAMHSA). Six key principles define trauma-informed practice. We can adapt these principles for UK schools. This builds supportive learning environments (SAMHSA).
According to research, learners need safety. They must feel physically and emotionally secure to learn well. Ensure predictable routines, consistent staff, and clear expectations. Create spaces without sensory overload. Van der Kolk (2014) shows safety unlocks learning, particularly for trauma-affected children.
2. Trustworthiness and Transparency: Adults are honest, consistent, and follow through on what they say. Decisions that affect the child are explained clearly and in advance. Avoid surprises where possible, and prepare learners for changes to routine.
These approaches also improve self-regulation (Perry, 2009) and reduce stress (Bomber, 2007). Learners benefit from peer support, a key protective factor. Circle time and buddy systems build connections. Collaborative learning helps learners develop social skills (Hughes et al., 2017).
| Tool | What It Measures | Who Completes It | Strengths | Limitations |
|---|---|---|---|---|
| SDQ (Strengths and Difficulties Questionnaire) | Emotional symptoms, conduct problems, hyperactivity, peer relationships, prosocial behaviour | Teacher, parent, or young person (11+) | Free, widely used in UK, quick to administer, validated for ages 2-17 | Does not specifically identify trauma; captures current symptoms, not causes |
| ACE Questionnaire | Ten categories of adverse childhood experiences | Individual (self-report) or trained professional | Directly measures adversity exposure; strong research base | Not designed for use with children; risk of re-traumatisation; does not measure impact |
| Boxall Profile | Developmental strands and diagnostic profile of social, emotional, and behavioural functioning | Teacher or key adult who knows the child well | Detailed developmental picture; directly informs intervention planning; widely used in nurture groups | Time-consuming to complete; requires training; licence fee |
4. Collaboration and Mutuality: Power is shared where possible. The learner has a voice in decisions that affect them, and their views are actively sought. This is particularly important for children whose trauma involved powerlessness or loss of control.
5. Choice: Offering meaningful choices, even small ones, helps restore a sense of agency. "Would you like to work at the table or on the carpet?" gives the child control without undermining the learning objective.
Consider historical contexts and cultural factors. Trauma manifests uniquely across cultures (van der Kolk, 2014). Check your biases to avoid re-traumatisation. Schools sometimes unintentionally harm learners from marginalised backgrounds (Bloom, 2010).
Research from Cole et al. (2005) shows trauma impacts learners. Focus on safety, connection, and emotional control. Use strategies which support these areas in your classroom, say experts.
Here are some practical strategies educators can use:
Researchers like Perry (2009) and Souers & Hall (2016) offer useful classroom strategies. These help learners heal, build resilience, and achieve success. Consider using these to improve outcomes.
Teachers: childhood trauma knowledge matters. Spot signs, use trauma-informed methods for safe learning spaces. Small actions help learners facing hardship (van der Kolk, 2014). A nurturing approach is vital (Perry & Szalavitz, 2006).
Trauma-informed schools need commitment and collaboration. Educators, families, and communities can help every learner thrive (Perry, 2009). Understand each learner's story, not just their behaviour (Bloom, 2010; van der Kolk, 2014).
Childhood trauma tests are screening tools used to identify potential adversity a learner has experienced. These instruments, such as the ACE questionnaire or the SDQ, help school staff recognise where emotional or social support might be necessary. They act as a starting point for further observation rather than a clinical diagnosis.
Teachers use these tools by making them one part of a broader safeguarding and support strategy. Screening is often conducted through structured questionnaires or during pastoral check-ins with the child. The information gathered helps staff adapt their approach to meet the specific emotional needs of the learner.
Identifying trauma allows teachers to move from seeing a child as difficult to understanding their behaviour as a survival response. This shift leads to more effective classroom management and a more supportive environment for the learner. When a child feels safe, they are more likely to engage with the curriculum and reach their potential.
Adverse childhood experiences may affect a learner's academic performance. Trauma can hinder a learner's focus, information processing, and emotional control (Hughes et al., 2017). Supportive adults at school improve outcomes for learners experiencing trauma (Anda et al., 2006).
One common mistake is using a screening score as a definitive label or diagnosis for a child. These tools are often limited and do not capture every type of adversity, such as community violence or poverty. It is also a mistake to ignore the role of protective factors, which can buffer the impact of high ACE scores.
A teacher should seek advice from a mental health professional if a screening tool suggests the trauma is severe or if the child’s behaviour remains highly distressed. Professionals can provide specialised therapeutic techniques that go beyond the support available in a standard classroom. Timely referral ensures that the child receives the expert care needed to handle their experiences.